History: We are the modern day inventors of the FUE procedure, doing these FUE procedures longer than anyone in the world, dating back to 1995. We published the first article on FUE in 2002 (https://baldingblog.com/wp-content/uploads/pdf/mp-2002-fue.pdf) and then the rest is history as doctors from all over the world started to do them. To encourage this technique, I handed out over 600 DVDs to the doctors at the International Society for Hair Transplant Surgeons meeting in 2002. This constituted a tutorial for the doctor and after viewing it, many doctors started to offer this technology to patients in their practice. The results of their initial results world-wide was Follicular Holocaust as most of the doctors failed to replicate what they saw in the technique on the DVD or in their patients who had the FUE procedure performed by them. Their failure rate, unfortunately, victimized many patients.
From this short term experience, Dr. Pak and I brought out of the closet the robot we built in 1998 and then added appropriate optics to the design and submitted two patents in 2003 on robotic hair restoration surgery technology. The patents were granted in 2006 so we are the patent holder inventors of the two core technologies of the hair transplant robot today. We proceeded to license a new start-up company, Restoration Robotics, who built the ARTAS robot from our core technology. The reason we invented the robot was because too many doctors failed to perform FUE successfully with the manual techniques I had developed, which is somewhat the case today. Since that time, significant improvements in the tools for FUE have been developed and the newest of these tools have been incorporated with our standardized techniques into our daily FUE offerings for our patients.
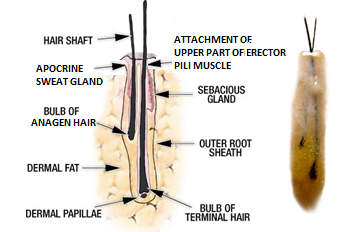
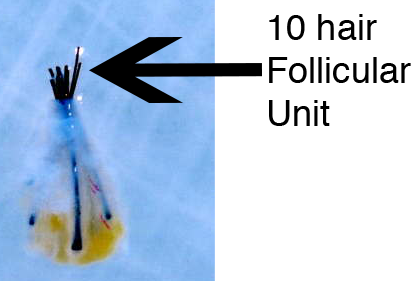
Take a careful look at the video after reviewing what I wrote below so that you can pick up on the nuances as each component of the FUE, which is very fast and difficult to see. What it shows is the use of a specialized punch as we align the punch to the center of the hair follicular unit under high powered optics. The punch is advanced at the proper angle, almost to the full length of the graft. In Caucasians, this length runs 5-6 mm on average, for the Asian, it may run 7-8 mm in length. What I defined in the article were insights into what can go wrong with FUE, for example, the presence of non-elastic collagen which may cause increased transection rates (amputation of the graft). Special skills are needed to avoid this. The FUE contains two direct steps that are unique to this type of surgery: (1) the coring of the grafts with an appropriate instrument, and (2) the plucking of the graft from the wound. Damage to the grafts can happen at both levels, first in #1, from mechanical damage from improperly aligned punches, the forces of torque which can cause tearing of the tissues during the coring phase and direct amputation of follicles in the graft from sharp punches.
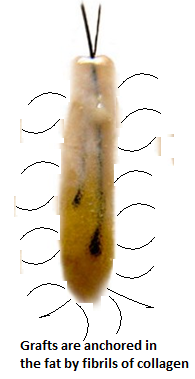
Hairs in the follicular unit graft are not always aligned straight, but may splay apart. This splay can cause the mechanical punches to amputate the hairs in the splay leaving you with less hair in each of the splayed grafts. When the grafts are plucked out, the tissue type of the patient (containing more or less elastic collagen in the graft which is different in each person) will cause either an easy pluck with minimal damage (with high elastin) or a difficult pluck (when elastin is low) which if not done carefully, will tear the follicle apart. It takes years to learn these techniques and novice doctors and novice teams working with these doctors takes years to really get it right.