This man posted his results from using Estrogen for 7 months on Reddit. His hair loss reversed. He claimed he was not a transgender, but I can’t imagine what it did for his sex life, beard, breasts and body hair. Balding isn’t that bad, is it?

This man posted his results from using Estrogen for 7 months on Reddit. His hair loss reversed. He claimed he was not a transgender, but I can’t imagine what it did for his sex life, beard, breasts and body hair. Balding isn’t that bad, is it?
This hairline is rounded as female hairlines should be. I have no way to tell if this is what the patient wanted for what the surgeon thought a male hairline should look like. The arrows indicate that the surgeon didn’t follow the preoperative plan. Technically, the transplant looks good but design wise, terrible for a male hairline (sourced from the internet)

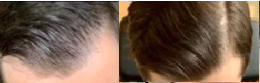
This is an outstanding result with reversal of the hairline corner loss in a short period of time


The hairline in this 25 year old male has clearly thickened up. I believe that he reversed the miniaturization at the hairline level
There is clearly an association between depression and the drug finasteride as shown in this article: https://pubmed.ncbi.nlm.nih.gov/33814544/
My goal would be to find a procedure that transplants clusters of hairs together, with a good amount of surrounding tissue, as some evidence is showing survival rates of those hairs fair much better when compared to single hairs that have been separated from the unit and transplanted. They specify that as 6-12mm.
Punch sizes of between 6-12 mm is way to big for FUE. The typical FUE uses 0.9 -1.0mm sized punches. All punch sizes even greater than 6mm were tried in the early days of hair transplantation in the late 1950 and 1960s. The oxygen never got to the hairs inside of the graft so that the only growth was on the rim of the graft, a donut shape hair pattern of growth. Then after I introduced FUE to both the ISHRS and published in a prominent journal, a demand for FUE appeared in the marketplace. The problem was that there were few good tools that everyone would standardize upon. Now there are a lot of different tools including dull punches, hybrid punches and round sharp[ circular punches are can remove grafts with a diameter as small as 0.8mm. Each doctor has their preferences. To get grafts with good tissue around them 100% of the time, if you don’t believe in FUE, you should consider a Strip surgery as the graft and its surrounding tissue and capsule are always harvested correctly. The FUE is a blind procedure depending upon unique surgical skills, good eyesight, and mechanical factors that allow the punch to successfully harvest the grafts, The grafts are 100% visible with the strip surgery because the follicular units can be seen (100%) under high powered microscopes. As far as clusters of hairs is concerned, the natural looking hair transplant uses only follicular units (clusters of follicular groups look like plugs), the normal anatomical grouping of the grafts, see photo below

I am 4 month post op after 2500 grafts and I have had it cut for the first time today grade 1 so it’s short and you can see the area where the surgeon has taken the grafts. I am fully aware how the transplant work and under no illusions the area won’t thicken out itself but I was under the impression the donor area wouldn’t be noticeable once healed. Is the donor area still healing? Has the surgeon taken too many grafts in a short area? It isn’t patchy just one big area going around the back and side of my head. I am hoping it isn’t noticeable when it grows a little more and maybe I can’t cut it too short anymore.
The number of grafts that are harvested and then produce a see-through donor area varies with (1) donor density, (2) hair shaft thickness and how many grafts were removed. Low original donor densities and super fine hair in combination can cause a see-through donor area with 2500 grafts harvested with FUE. Your surgeon can discuss risk with you and your specific situation
Do we know how transplanted will look like 60 years after they are transplanted!
We know that these transplants can last more than 40 years as the commercialization of hair transplantation happened in the late 1950s in New York. These original transplants didn’t look good, but they lasted nevertheless. I think that Joe Biden’s original hair transplant is more than 40 years old and makes up the bulk of the hair that he has not in the front of his head
Amazing reversal of advanced hair loss pattern with minoxidil and finasteride alone. This degree of reversal is unusual but very welcome I am sure


Low T symptoms have been bothering me for 5 years in such a way that I lost all ability to function normally. I am pretty much set on it starting it soon, but my only concern is losing hair on it. I am NW0 and have pretty healthy-looking hair for 31 year old, but still would not like to lose it. I know fin + TRT could pretty much be in conflict with each other, but my low T symptoms are so severe that I think I would let my hair go if I could function normally again.
If you don’t have the balding genes, you probably will not lose hair by taking exogenous testosterone. Also, if you don’t have the balding genes, you don’t have to take DHT blockers like finasteride or dutasteride
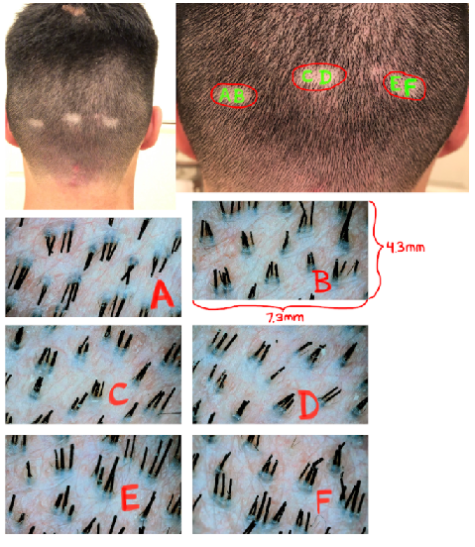
Let me tell you what I see. I see some normal hairs (the thick dark ones), some thinner dark one as well (undergoing early miniaturization) and some skinny almost dark hairs (more advanced miniaturization) and some threadlike hair (end stage miniaturization just before these hairs will fall out and not regrow). I can’t properly count them and quantify the degree of miniaturization because they are disorderly. If the hair was cut short, this is what I might see (not you of course) in the second picture. From that I can determine (1) the total hair count you were born with, (2) your donor density, (3) your lifetime graft supply for hair transplant and (4) if you have DUPA or not

There are many triggers such as extreme weight loss, illness, major surgery, drugs, and a variety of diseases of the scalp with quick or slow onset and genetics for men and women.
I understand that fraternal twins have completely different genetics (unlike identical twins). However, from your experiences with patients, if one fraternal twin is suffering from MPB at a young age (20), will the other twin be more at risk to suffer from hair loss in the future?
That is not true. The genes for balding might have been inherited in only one of the twins. The risks, depending upon the family genetics, can be very different for the second fraternal twin. If they were identical twins, then they would both bald of not bald in the same way. I had a pair of twins, where one lost more hair faster than the other. Stress and hair systems was the cause for the twin that lost much more hair than the other twin.
My hair started thinning (diffused) in my 30s, and really took a turn for the worse the last few years. I still have most of my hairline (it’s receded some). I used to do the rogain foam, but that tanked my blood pressure so i had to stop. My question for you is: what kind of results can i expect on fin at my advanced age?
Usually, finasteride works best when the hair loss is recent (past few years). In a 45 year old male, the hair loss may have started in your 20s, which would reduce the expectations, except possibly in the crown. If you started balding recently, then the odds work in your favor. In your case, the past few years of lost may be where your benefits lie.
It’s been reported that Dutasteride raises scalp Testosterone by nearly 100%. I don’t know if thats bro science or what. When I took fin for 10 years, my hair line didn’t move a cm. Since taking dut for 7 months, my hair line has went from a thick NW1 to an approaching NW2.5-NW3. I can see the pattern taking shape, although I’m about a NW1.5 now. Can Scalp Testosterone cause damage to hair follicles, particular the front where they may be more sensitive to T in general? Thinking of going back to fin and cutting my losses. Enough is enough
The model for hair loss is for DHT, which is a metabolite in the breakdown of testosterone by the body. Norwood Class 1 and 2 have juvenile hairlines and the leading edge of these hairlines do not respond to DHT blockers like finasteride, so using drugs to hold onto your juvenile hairline makes no sense and just will not work.