Yes, some people get changes in mood on finasteride. That is a problem for men with depression as it could exacerbate it.
This is a case of necrosis. I don’t understand why it keeps happening in Turkey. In my 33 years in practice, as the first surgeon to do 5000 grafts and as the pioneer of FUE, I have never seen this complication. These three pictures show the progression of the necrosis over time and the final scarring that resulted. I see other areas where there is a suggestion of further compromise. These scars will not grow the transplanted hair. Another hair transplant by a competent surgeon may fix this problem.

So I had my hair transplant done on Jan 2nd. I had virtually no shedding in the past 1 months but I started using topical Minoxidil a week ago and all of a sudden got dandruff in the transplanted area. My doctor told me to scrub it off and I did and gave him some after pictures with some hair down the drain. My questions:
I did this after 4 weeks. I was told it takes 2 weeks for the hair to root. Did I accidentally peel off some hair or was the shedding at the same time?
How do confirm what I shed was legit or I accidentally messed up transplant?
I’m worried. I have had no problems so far and was going so far with maybe a hair or two in the drain. Pictures attached! If it’s just shedding it couldn’t have been timed worse. Stats: 2100 transplant count Age: 36
Scrubbing your transplanted area after 12 days will not cause loss of the implanted hair stem cells that, I expect, will eventually grow. Starting minoxidil could induce some shedding, which tells you that the drug may be working to develop new hair in the non-transplanted areas. I believe that you don’t really have a problem.

4000 grafts are likely 60% or more of your donor supply. Have you considered what you would do if your hair loss pattern evolved into a more advanced balding pattern? If you are under 26, this is a significant question; however, if you are over 35, the risk of developing a more advanced pattern may not be substantial unless some male in your family line developed a later pattern of advanced balding. Who do you take after in your family line? Do you have a worst-case plan? I think 4000 grafts for a balding Class 3 pattern male is mal-practice.
Do hairs like this stand a change with medication? Is a HT even a viable option to increase density?
Because of the possibility of diffuse unpatterned hair loss, I would want to look carefully at your donor area with a hand microscope to make sure you don’t have DUPA, which will rule out a hair transplant that probably would fail if you have DUPA. Medications may work well but have the medications managed by a good, caring, competent doctor

Finasteride can positively impact a swollen prostate and is typically used in men with prostatic hypertrophy, commonly over the age of 50. Also, in men who used it for a long time, it reduces the risk of prostate cancer by 25%. The recommended dose, however, is 5mg, in the form of Proscar.
I think that 23 years of age is too early because your final balding pattern doesn’t usually show up until you are 25-26 years of age, and even at 26, it may not show up. When I do a hair transplant, I prefer men over 25. The number of grafts depends on four factors: (1) the size of the area being transplanted, (2) the location of the transplant (frontal hairline or not?), (3) your donor density, and (4) your hair mass per unit hair. With that, I can build a personalized Master Plan for any patient, which will consider what might happen to them as they continue to bald (as every man who is balding does).

The doctor should discuss a plan when he/she intends to harvest hair outside of the donor area, as shown in this picture. A procedure with 4500 grafts and the harvesting FUE patterns shown demonstrate the problem. If his balding pattern increases, many transplanted hairs will fall out because many hairs/grafts were taken outside the safe donor area. FYI: The safe donor area is a 2 1/2 – 3-inch high area from the base of the skull around the side of the head above the ears to the temple peaks.

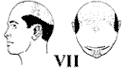
The evidence I’ve compiled indicates that Donald Trump exhibits a Norwood Class 5-7 balding pattern (the Class 7 pattern is depicted below). It appears that he underwent multiple surgeries, leading to the relocation of much of his remaining hair to conceal the frontal and top areas, albeit with limited success. Since Propecia was not available when he underwent scalp reduction surgery in the early 1990s, most men undergoing such procedures or hair transplants before 1997, when Propecia first came to the US market, experienced accelerated hair loss progression. Unfortunately for Mr. Trump, this would likely result in the development of an advanced pattern, such as the Class 7 pattern illustrated in the following graphic.
 “New York City-based cosmetic surgeon Gary Linkov believes that the politician may have undergone five separate hair-transplant surgeries” (https://www.newsweek.com/donald-trump-five-hair-transplants-gary-linkov-1832991). I know that Donald Trump received Scalp Reduction Surgery sometime in the early 1990s when this barbaric surgery was a standard treatment for hair loss found in the top and crown of the head. I know its barbaric nature because I had three of these procedures over 90 days. By its very nature, Scalp Reduction Surgery attempts to surgically remove the bald area, stretching and thinning the donor area (the rim of hair around the head). Add to that the claim by Dr. Linkov that he believes that Trump had 5 hair transplant surgeries, likely in 1990 (before FUE was invented), suggests that most of his residual native hair (that should reflect a rim of thick hair going around the back and sides of the head) was moved into the balding area, thereby depleting his natural rim of hair from his balding pattern.
“New York City-based cosmetic surgeon Gary Linkov believes that the politician may have undergone five separate hair-transplant surgeries” (https://www.newsweek.com/donald-trump-five-hair-transplants-gary-linkov-1832991). I know that Donald Trump received Scalp Reduction Surgery sometime in the early 1990s when this barbaric surgery was a standard treatment for hair loss found in the top and crown of the head. I know its barbaric nature because I had three of these procedures over 90 days. By its very nature, Scalp Reduction Surgery attempts to surgically remove the bald area, stretching and thinning the donor area (the rim of hair around the head). Add to that the claim by Dr. Linkov that he believes that Trump had 5 hair transplant surgeries, likely in 1990 (before FUE was invented), suggests that most of his residual native hair (that should reflect a rim of thick hair going around the back and sides of the head) was moved into the balding area, thereby depleting his natural rim of hair from his balding pattern.
Photos of Trump boarding Air Force One reveal that the back of his head doesn’t seem to have much hair, suggesting minimal hair in that area where he should have had a strong rim of hair 3 inches high. Additionally, recent footage this week shows exposure of his frontal hairline, a characteristic often associated with wigs (hair systems). It’s common for such hair systems to be secured using glues, weaves, and hair clips. Considering the cumulative evidence of (1) the lack of hair at the back, (2) the exposed scalp in the front as what appears to be the lifting of his hair system from environmental factors like wind, and (3) the use of clips behind the ears used to secure a hair system in place, (4) the effect of multiple hair transplants on a Class 5-7 patterned balding man’s rim of hair, and the difference in color of the side hair (gray) from the top hair (blonde), it’s reasonable to conclude that Mr. Trump likely uses an expensive hair system. This system may involve gluing it to his scalp, weaving it with residual native hair, and using hair clips to secure it on the sides, where most of his remaining hair is likely located. Such hair systems often require regular adjustments every 2-3 weeks to accommodate the growth of native hair and then reattaching them. The hair is synthetic or human hair used to make hair systems and is often fixed on a lace platform, which is then glued to the scalp. The effects of these ‘lace’ systems are very effective if you maintain them properly. I have seen him pull back his hair in front of a camera on a late-night TV program that looked completely normal, consistent with a lace hair system.



The above photo reference showing his frontal scalp, see here: https://www.msn.com/en-ca/news/politics/concerns-raised-for-trump-s-hair-after-it-is-seen-flapping-in-the-wind/ar-AA1nHveb?ocid=mailsignout&pc=U591&cvid=2dc0422ef6d34569b9baf6f70de0fac9&ei=32
Below are some other interesting posts on this subject:
Minoxidil will have no value to the transplanted hairs. Minoxidil’s has value is in the non-transplanted areas. I performed a study where I had patients apply minoxidil to 1/3rd of the transplanted area (to manage overlap) and then compared both the speed of growth and the thickness of the end result. There was no difference between the treated sides and the non-treated sides.
The use of both of these topical medications is effective, as shown here; however, a considerable amount of both of these drugs go systemic. It would be easier to take them orally and then you would know the systemic component of the dosage.

Many men have written to me to ask me if they had Diffuse Unpatterned Alopecia (DUPA), which I defined in the literature with Dr. Bob Bernstein in 1996. This is a “female type of pattern” where the hair in the donor area has significant miniaturized hairs. In men, it is also called Senile Alopecia when appearing in aging men, but here, the hair is uniform in thickness, so miniaturization is not present. The basic premise in hair restoration surgery is that the donor area (a rim of hair about 2 1/2 inches above the ears and around the base of the skull) is privileged hair protected against the genetic of balding. The Norwood Classification shows this area in the Class 7 patterned patient.
The diagnosis is critical because the donor area is no longer protected from the balding process. We don’t believe that DUPA is necessarily inherited, but we don’t know. Sometimes, this donor area miniaturization will respond to finasteride but often does not. If any surgeon dares use this as a source of hair for a hair transplant, the hair transplant will fail, which is a classic malpractice, in my opinion. But for those impacted, controlling their hair loss becomes a real challenge. We have seen the existence of genetic patterned hair loss with DUPA also present, so these men are unfortunately double challenged.
This link shows a classic case of DUPA (https://baldingblog.com/do-i-have-dupa-photo/), so I ask all of my patients to get a hand microscope and cut the hair short in the area, just enough to use the hand microscope and get a good picture as shown in the above post.
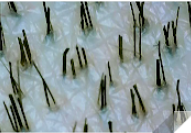
Another man just wrote to me, got a hand microscope, and showed me photos of his donor area. I told him he didn’t have DUPA now, without a doubt. See the photos he sent me below. Very few miniaturized hairs are present, certainly not enough to reach the 20% threshold I use to diagnose DUPA.
I was told that I haven’t lost enough hair to fill in the highlighted areas where I’ve been balding (see outline of my thinning). Do I need to loose more hair to become a better candidate? I consulted two clinics about the number of grafts for my hairline. One said 2000 the other said 2500-2800. Above 2000 seems like too much to me, but I’m not sure. Any feedback is appreciated.
Why undergo a hair transplant if you don’t need it? Hair transplants accelerate balding, especially in younger men. You would likely lose much of the hair presently on your head if there is significant miniaturization present, so maybe a transplant would be switching from what you have to transplanted hair with marginal gain other than the surgeon making money at your expense. There are great medical treatments for your hair if you think you are thinning. Get a doctor that knows how to treat you medically.

I waited for 12 days before washing the recipient area of my transplant. At that time, could I have damaged the grafts?
We wrote an article that discusses what happens day by day after a hair transplant. The grafts are secure in 7-8 days if no crusting is present. If crusting has not come off with good washing, removing the crusts at 12 days with good washing techniques is safe.
I’m 35yrs old living in South East England. Started receding about 10yrs ago and never done anything to prevent it. Only recently started considering a transplant as I’m now starting to be able to afford it.
Your worst-case balding pattern is a Norwood Class 5A pattern. These patterns are suitable for a surgeon to work with because they usually don’t progress to a Class 6 or 7 pattern (no guarantee of course). The key is to get a good assessment of your donor supply (donor density and hair thickness), and then., if you use a good, honest, artistic surgeon, you can get a good estimate for the work. There are many good UK Surgeons who can do this with creative and artistic skills.
