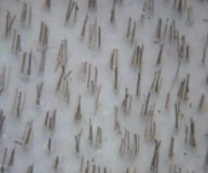
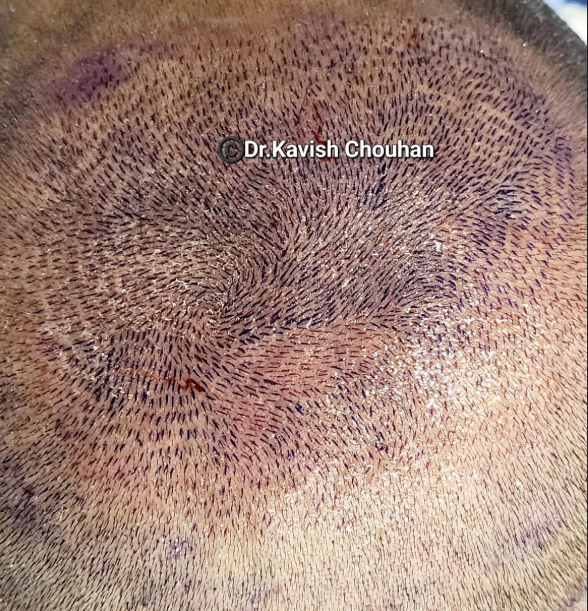
At the bottom of this posting, there are two examples of views of the donor area under a hand microscope (these can be purchased on Amazon.com). The microscopic view on the picture above averages about 2 hairs per follicular unit. This number is close to the average Caucasian’s density with a total hair count reflecting 100,000 hairs on the head. The picture below shows follicular units that contain far more than 2 hairs each (a very high donor density). Without calculating it but eyeballing it, it appears that the number of hairs exceeds 3 hairs for each follicular group or more than 150,000 hairs on the head. Let’s assume that there are 3 hairs per follicular unit for the simplicity of the calculations that follow.
The average human has 50,000 follicular units on his hair-bearing scalp, averaging 2 hairs each, which calculates to 100,000 hairs on the head. If you look at the Class 7 balding pattern patient, the remaining hair is the only hair that we can legitimately call permanent hair. This reflects 20% of the hair-baring surface on the scalp (excluding neck hair), i.e., in a typical Caucasian male, 20% of the 100,000 hairs are permanent hairs for transplantation, which is 20,000 hairs or 10,000 permanent Follicular Units (grafts). That means the area would be completely bald if 10,000 grafts were taken out of the Class 7 patterned area. Therefore, the obvious question is how many grafts of these 10,000 permanent hair Folliclar Units (grafts) we can move. The answer depends on a series of factors, but if you have medium-weight hair (50 microns thick/hair), you can safely move up to 60%, or 6,000 grafts with the FUE technique. If your hair is more coarse, the number of harvestable grafts can be higher so that the remaining follicular units (grafts) will be enough to make the donor area look normal as the hair mass is what determines if you are overharvested. Coarser hair has a higher hair mass than medium-weight hair. However, if the hair is fine, the number of safe extractions will drop below the 6,000 Follicular Units (grafts) that can be safely harvested because if you removed 6000 grafts with fine hair, the residual donor hair mass might not be enough to prevent a see-through donor area. When you or your surgeon push these numbers higher (assuming your hair is fine), you take a risk of donor area depletion, which produces a see-through donor area (i.e., balding in the donor area). This is why I am writing this post, to give you, the reader, the power to understand the logic in the decisions on estimating the maximum number of grafts you can move before risking a see-through donor area.
20% of the 100,000 hairs are permanent hairs for transplantation, which is 20,000 hairs or 10,000 permanent Follicular Units (grafts). That means the area would be completely bald if 10,000 grafts were taken out of the Class 7 patterned area. Therefore, the obvious question is how many grafts of these 10,000 permanent hair Folliclar Units (grafts) we can move. The answer depends on a series of factors, but if you have medium-weight hair (50 microns thick/hair), you can safely move up to 60%, or 6,000 grafts with the FUE technique. If your hair is more coarse, the number of harvestable grafts can be higher so that the remaining follicular units (grafts) will be enough to make the donor area look normal as the hair mass is what determines if you are overharvested. Coarser hair has a higher hair mass than medium-weight hair. However, if the hair is fine, the number of safe extractions will drop below the 6,000 Follicular Units (grafts) that can be safely harvested because if you removed 6000 grafts with fine hair, the residual donor hair mass might not be enough to prevent a see-through donor area. When you or your surgeon push these numbers higher (assuming your hair is fine), you take a risk of donor area depletion, which produces a see-through donor area (i.e., balding in the donor area). This is why I am writing this post, to give you, the reader, the power to understand the logic in the decisions on estimating the maximum number of grafts you can move before risking a see-through donor area.
One reality is that most people don’t bald to a Class 7 pattern (only 7% of the male population), but might stop at a Class 6 pattern of balding, so if you and your surgeon decide that you are willing to extend the donor area to the Class 6 pattern of balding, then the number of permanent  hairs will increase to 30,000 hairs, and the number of harvestable grafts will be much higher with harvestable grafts (assuming that your hair is medium weight) to possibly at 9,000 Follicular Units (or grafts) leaving 6,000 remaining follicular units to cover the donor area (this is the size of the Class 6 pattern of remaining hair). The decision to increase the projected size of the donor area has its risks because no one will know for sure that they will never develop a Class 7 pattern. The consequences of this decision is (1) the extra 3,000 transplanted grafts will not live and might die if you develop a Class 7 pattern of balding, and (2) the harvested area will show with FUE white scars which will be visible to others. So this decision should not be taken lightly and it must be discussed with your doctor at the time of the FUE, or you may regret the decision sometime in the future.
hairs will increase to 30,000 hairs, and the number of harvestable grafts will be much higher with harvestable grafts (assuming that your hair is medium weight) to possibly at 9,000 Follicular Units (or grafts) leaving 6,000 remaining follicular units to cover the donor area (this is the size of the Class 6 pattern of remaining hair). The decision to increase the projected size of the donor area has its risks because no one will know for sure that they will never develop a Class 7 pattern. The consequences of this decision is (1) the extra 3,000 transplanted grafts will not live and might die if you develop a Class 7 pattern of balding, and (2) the harvested area will show with FUE white scars which will be visible to others. So this decision should not be taken lightly and it must be discussed with your doctor at the time of the FUE, or you may regret the decision sometime in the future.
In the microscopic view of the patient on the right (pictures below) who shows a very high donor density, the harvestable hairs in the Class 7 area may have doubled because the look of the donor area reflects not the number of hairs that were removed, but rather the number of hairs (or follicular groups or grafts) left behind. To calculate the safe harvestable number of grafts, the key is to leave behind approximately 4000 Follicular units. With an average Follicular Unit density of 3, the donor area contains 30,000 hairs or 15,000 Follicular Units (grafts) so that to leave behind 6000 grafts, this patient can safely harvest 9000 Follicular Units (15,000 – 9,000 = 6,000).
The use of strip surgery, on the other hand, always keeps the excised donor hair at the lower side of the Class 7 permanent zone, so that if your surgeon and you decide to take more grafts, other than a risk of creating a scar, the risk of placing non-permanent hairs with the surgery is very low and the risk of seeing an area of harvested grafts with no hair will likely not occur. Of course, the risk here is potential scarring. The use of “Scalp Micropigmentation” solves the problem for either a see-through donor area or a scar. Here are examples of what can go wrong if things are not done right: https://baldingblog.com/collection-victim-photos-internet-harvested-depleted-donor-areas/