Is reversing premature greying possible with Palmitoyl Tetrapeptide-20?
It seems to have value, according to what I have read.
Is reversing premature greying possible with Palmitoyl Tetrapeptide-20?
It seems to have value, according to what I have read.
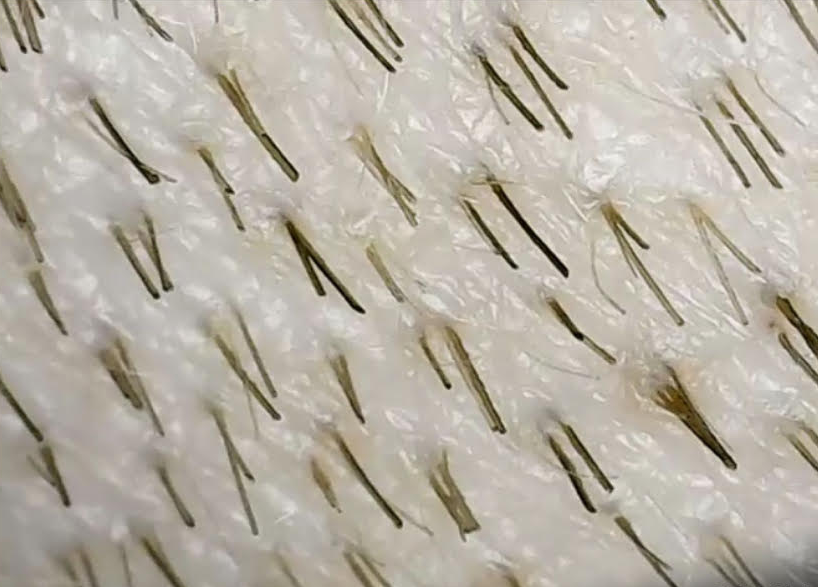
I am scheduled for an upcoming hair transplant, and I am worried about having Diffuse Unpatterned Alopecia (DUPA). The surgeon didn’t understand when I asked him about DUPA in my donor area, and I don’t want to go forward if I have DUPA. Please help me with the diagnosis. Here are four pictures from my donor area.
The first picture qualifies for DUPA as there are many hypopigmented hairs in the field of view. The other photos show a much more straightforward case of DUPA. I define DUPA as miniaturization over 20% of the hairs in the donor area. The third photo shows well over 20% miniaturized hair, which you can count easily. I would want a more extensive evaluation of the donor area before tackling a hair transplant, but what is here strongly suggests DUPA. He met face-to-face with three doctors before speaking with me by phone. Shame on the doctor for (1) not understanding his concerns about DUPA, (2) not listening to his concerns, and (3) not making the diagnosis when he was before them. Some doctors just do this for the money and really don’t care what happens to these patients after the surgery. I tell the patient to ask himself the question: “Is this a doctor you trust?” This is a critical question everyone should ask before allowing them to work on their scalp.
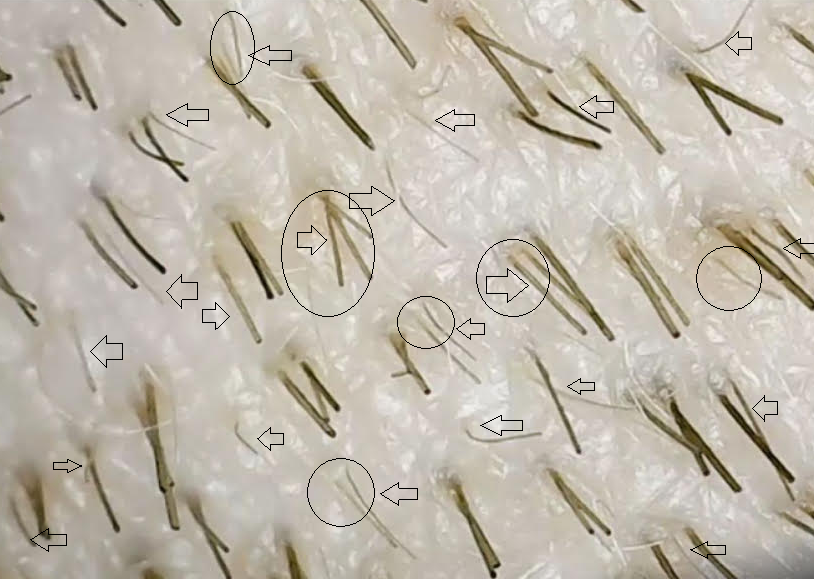
I outlined in a circle (the third picture is the same photo as #2) with arrows and circles showing the hairs in the field that I think are miniaturized. As this is part of the donor area, it would worry me a great deal if a hair transplant was on the agenda unless, that is, a better and more comprehensive assessment of the donor area is performed. Click on the photo to enlarge it.
Dr. Robert Bernstein and I discussed DUPA and concluded that Finasteride works in most men to some degree. It is worth trying this for a year and then reassessing the patient’s situation as having great before pictures is invaluable.

I’m thinning in my crown area so it’s not easy to see the progress I’m making. So I decided to purchase a microscope for inspecting the scalp. I didn’t know I could get these on Amazon for couple of bucks. It was pretty fun looking at my scalp so close. The picture shown here is my crown area that’s thinning. I can definitely see a lot of things going on there. I’m on fin and oral min so I’m hoping those drugs will reverse the process I am seeing.
The picture of the crown shows significant hair loss, with many follicular groups having only one thicker and one thread-like hair (a remnant of the hair that used to be there). Some of the follicular groups have both hairs impacted and threadlike. This single photo shows almost all of the stages of the hair loss process. This active balding process will eventually lead to the remaining hairs thinning and possibly falling out.
I’m 25M I made a post a long time ago talking about my nonfin hair loss stack. It was actually working decently well for me but I got tired of using so many topicals so I just switched to Fin + min only. Ive been on that stack for about 6-8 months now. I don’t have a before or after because there’s been no drastic changes really. I’m maintaining but I’m way more carefree about my hair now. I used to not style it for years or blow dry it because I was scared it would make me lose hair faster. I was trying to change my lifestyle & do things like avoid coffee to try to slow or stop my hair loss
Now I just take my fin & do what I want with my hair. I actually style it when I go out now and I like how I look. I still have my insecurities but fin has definitely helped. I love the drug. It’s given me more confidence and that’s all I could ask for. I do have some side effect, which are quite manageable. The are: 1) Watery semen (by a little), 2) Nipple sensitivity, 3) I had an increase in sex drive at the start, slight decrease in sex drive now but I’m also cutting weight so that could be a contributing factor
This is not an atypical story. Most men with good results, just don’t talk about it, but bad results is like the news, everyone wants to hear about bad results from medications or even hair transplants.
Will Minoxidil stop irreversible hair loss if I stop taking Fin when trying for a baby?
The mechanisms of action of these two drugs are very different. If you had a successful experience with finasteride, stopping will cause you to lose all of its benefits, and I would not expect minoxidil to rescue you. Minoxidil can produce hair, but certainty and timing are two variables that might not coordinate with your desire to conceive a baby.
I (F27) have recently moved to UK . I don’t know if it’s the weather change or the water but I am losing a lot of hair. The wash days are an absolute nightmare. If this continues I believe I might go bald. If any kind soul here can suggest what can I bring in my hair routine to stop this severe hair fall and promote regrowth. I want to avoid surgery or transplant as much as possible.
What you describe is stress and stress hair loss can produce a telogen effluvium, reversible over time in most young females. You should see a dermatologist to manage your hair loss.
How often should it be done? I’ve seen lots of different suggestions e.g. twice a week, once a week, once every 2 weeks, once every 3 weeks, once monthly etc
I believe that microneedling should be done once a week. The purpose of microneeding is to create a wound and a healing cascade which generally cycles in one week. More often doesn’t do any good.
I’m 25 and I have a Norwood 2 and I’m just wondering at what age is your final Norwood apparent or predictable?
For most men, hair loss patterns can be picked up by the age of 26 with proper tools (Microscopic imaging and micrometers); however, this is not a 100% rule as I have seen men start their balding in their 30s, 40s, and even in the 50s.
If most hair loss occurs by 35 and then pretty much stabilises does that mean we can stop taking fin after 35?
Hair loss is progressive. If you are stable on finasteride, stop it, and you might find instant hair loss to a pattern that you should have had if you didn’t take finasteride. I call this “Catch-up Hair Loss,” which means that you lose all of the benefits plus what you fixed by going on the drug. Catch-up Hair Loss always occurs in men on long-term finasteride. This is a warning for you: don’t do something that you might regret, as so many people I have taken care of told me when they decided to stop taking finasteride.
Hello Dr Rassman, I have a question. I am on 5mg of oral Minoxodil a day. I have been told by a few people it may be too much. Thing is, my hair is not getting better. Been on it for 8 months, hairloss is rapidly increasing to the point I am nearing NW3 when I was barely even NW1 8 months ago (Shedding hundreds of hairs over the sink) My question is, if I lower my Minoxodil dose to 2.5mg every day, will that cause even more hairloss? I’m worried about being stuck on 5mg of minoxodil for the rest of my life
This is a balancing act between safety and effectiveness. Lowering the dose to 2.5mgs shouldn’t have an impact on you; however, with continued shedding, maybe finasteride is worth considering
Some evidence suggests that taking Ozempic causes individuals to experience telogen effluvium. We see Telogen effluvium when there is rapid weight loss, particularly in people who are not balding; however, those individuals with genetic balding who undergo rapid weight loss can accelerate their hair loss, significantly impacting miniaturized hairs on the head. If it is just a telogen effluvium, then it probably will reverse when the rapid hair loss stops, but if it impacts miniaturized hairs, these hairs may not return. It is also known that rapid weight loss can impact thyroid function, another thing to worry about.
A hair transplant is a significant decision that should not be taken lightly. Most importantly, you must realize that hair loss is a progressive process, so getting a hair transplant may not solve your hair loss problem down the road. When considering a hair transplant, you must know (1) the worst-case badling pattern that you might end up with, (2) your donor supply i.e. how many grafts do you have in your lifetime to cover future balding? (3) how many grafts are you going to use now? (4) when will you deplete your donor supply such that it, too, will become see-through or significantly bald? (5) what is the quality of your hair (individual hair thickness) in the donor area, hair character (curly vs straight), and lastly what is the color contrast between your hair and skin color? Many undertrained doctors, and especially technicians who mostly need help understanding what I am talking about (above), are the ones who are doing surgeries in Turkey for the money. Many of these surgical technician-run clinics (some have doctors who front the process) are destroying the donor area and failing on the hair transplants, damning their victims with (a) terrible results, (b) not enough donor supply left to fix the failed hair transplant and (c) balding or bald donor areas. I hope that those of you considering a hair transplant find a good surgeon who understands all of the above and can give you the confidence of a long-term Personalized Master Plan, which is what I have done for all of my surgical patients throughout my career.
What is the long term perspective for someone who responds to common treatments like fin and min? Lets say a person starts these treatments at 30. Will they preserve their thickness into their 50s and 60s? Or they just delay the inevitable balding by 5-10 years?
I have been in the hair restoration field for 33 years and have seen it all. Men on Finasteride for life see a reduction of their end-stage bading pattern. Although the hair loss process continues, it is slowed down significantly with age. I have patients that have been on finasteride 25 years, and a few decided to stop it only to find significant hair loss occurs within 3 months of the date they stopped the drug. The same can be said with minoxidil or both in combination.
I’ve been using topical minoxidil and oral finasteride for around 6 months. My loss has pretty much stabilized but no regrowth so far. I’m thinking about switching to oral minoxidil. Is this a good idea after 6 months or should I wait longer like with finasteride? Also, I have a lot of body hair, basically all over (shoulders, back, chest, stomach, you name it). I guess this can’t even get much worse with oral minoxidil, just wondering if anyone else who already had a lot of body hair here started using oral minoxidil and what their experience was.
What do you think? Switch now or wait longer?
if you feel that minoxidil is not working, then you probably do not have Sulfotransferases, an enzyme that enhances the conversion of Minoxidil to Minoxidil Sulfate, the active form of minoxidil for hair growth. Sulfotransferases are found both in the liver and in the ‘outer root hair sheath’ of the hair follicle. When present in the hair follicle, the person will respond well to minoxidil. Only about 40% of people are responders to minoxidil in the scalp. Because it is also present in the liver, the conversion of oral minoxidil to minoxidil sulfate in the liver with the oral minoxidil may help people who do not have this enzyme in the scalp hair follicles, making them more responsive to oral minoxidil than to topical minoxidil. That becomes a decision that only you know if the topical minoxidil is working, if not, then the switch may be a reasonable decision.
The following is the introduction of the article titled: Pericardial, pleural effusion and anasarca: A rare complication of low-dose oral minoxidil for hair loss
Authors: Ncoza C. Dlova, MBChB, PhD, Tarryn Jacobs, MBChB, and Satish Singh, MBChB
“INTRODUCTION
Topical minoxidil has been used for many years in the treatment of androgenic alopecia and other hair disorders. Although the mechanism of action of topical minoxidil is poorly understood, animal studies have shown that it affects the hair growth cycle by shortening the telogen phase and prolonging the anagen phase.1,2 Lately, there has been growing evidence to support successful use of low-dose oral minoxidil (LDOM) in the treatment of various types of alopecia. The dosing regimens range from 0.25 to 5 mg daily to twice daily, with side effects reported to be dose dependent.”
The presented Pericardial Effusion occurred 3 weeks after starting the low-dose oral minoxidil. The woman presented with significant swelling in her feet and eventually elsewhere. A Pericardial Effusion is a condition where fluid accumulates around the heart, inside the sac (pericardium) that surrounds the heart. Fluid in this space will restrict blood flow to the heart and fluid back up in the body. Significant swelling of the feet and anasarca (a generalized swelling of many body parts) was clearly a warning that brought this woman to a doctor. She was admitted to the hospital, treated with diuretics, and stopped the oral minoxidil, all of which normalized her state of health, so she was discharged from the hospital on the 5th day.
WARNING: People taking oral minoxidil or even high-dose topical minoxidil might develop the symptoms described above. Always seek medical attention when a change in your health to this magnitude appears, especially if you are taking oral minoxidil.
Ref: JAAD Case Reports 2022;28:94-6., 2352-5126, 2022 by the American Academy of Dermatology, Inc. Published, by Elsevier, Inc. This is an open-access article under the CC BY-
NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). https://doi.org/10.1016/j.jdcr.2022.07.044