Fantastic response from finasteride in just one month which shows that this man is exquisitely sensitive to finasteride. The miniaturized hairs quickly grew into terminal hairs.


Fantastic response from finasteride in just one month which shows that this man is exquisitely sensitive to finasteride. The miniaturized hairs quickly grew into terminal hairs.
The distribution of your hair in hair grafts in a Class 7 pattern is dependent upon (1) your donor density (available supply of graft without depleting the donor area, (2) your styling preferences, (3) the thickness of your donor hair (Hair mass of each shaft which is a measurable criteria) and (4) your pocketbook. A good doctor should be able to set up realistic expectations for you here. You must recognize that the bald area is three times the area of your entire donor area and that only a little over half of your donor area can contribute grafts to the bald area which means that a little over 1/5th of the hair is movable to cover an area 5 times the size. Anybody can figure out that the math doesn’t work, so how do you get good results when there is such a limitation? That is the ART that the doctor does the surgery with a good design and an understanding of what he has to work with and what he can and can not accomplish. The key is to communicate this information to you, the patient.
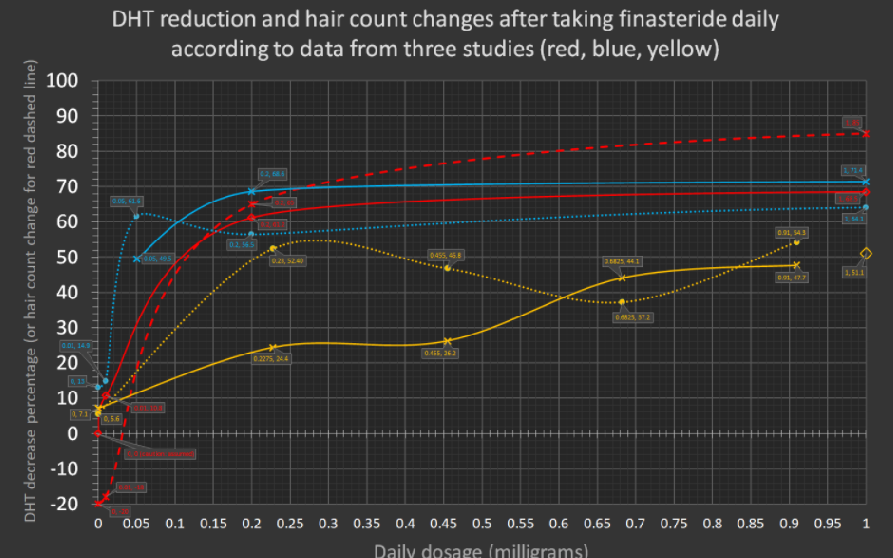
The following is from a Reddit post. The graph is very interesting. I asked for the references from the poster for scientific clarity:
BACKGROUND: Many of you will be familiar with this old graph showing DHT inhibition from various microdoses of finasteride. You may even be using that data to help you choose which microdose of finasteride to take in an attempt at minimizing the chance of side effects. Turns out it was derived from the study: “Clinical dose ranging studies with finasteride, a type 2 5cz-reductase inhibitor, in men with male pattern hair loss”. However, as far as I can see, the graph isn’t actually displayed in the original study. Someone created the graph from just the numbers that the study reported.
Anyway, the home-brew graph contains a number of limitations, so I’ve improved upon it in the following ways:
Instead of using just one study, mine uses three, one of which is topical. That’s all of the range dosing studies as far as I know! They are colour coded everywhere in the image for clarity. The old graph is represented in my new graph as the red solid (not dotted) curve.
The graph display range has been adjusted from 0-5mg to 0-1mg. This helps make it a lot easier to see the much smaller microdoses, even around 0.05mg.
I give the ORIGINAL data points (as shown by the diamond/circle/X points and x/y labels). Needless to say, everything else is derived and only an approximation, so should be treated with caution!
Accuracy is better in the new one. The old one has a figure of 25% DHT inhibition for 1/16th mg dosage. I think the true figure is more like 37% as shown in the new graph.
I also give (where applicable) the DHT percentage reduced not just in the serum, but also the scalp, and also show a curve reporting the number of hairs grown back (or lost) – see the dashed red curve.
Finally, the studies I used are listed, and I stated the number of days / months before a DHT measurement is taken.
As more microdosing studies come in (topical or oral), I look forward to updating the graph further. Here’s the new graph again: https://archive.is/OGDk3
Click to enlarge
I had a small thin spot on my crown that I’d like to darken with smp while I wait for possible results on finasteride. I was considering temporary smp. What do you recommend? I’m 25 with hairloss only in the crown, 6 months on fin. Thank you
We don’t do temporary SMP, but many people who had it grew their hair without it being detectable. We actually offer it for hair transplant patients who may not be as full as they want.
I’m 23M male with MPB. Currently I’m NW2 however my forehead has always been huge, it’s part of my skull structure. The question I’d like to ask is: does this procedure usually cause shock loss of the hairs (at the hairline or all over the scalp)? I need to reduce my forehead’s size (not my hairline) Thank you
23 year old men should not, in my opinion, get a forehead reduction surgery because of the risk of further recession and balding. You don’t know your balding pattern or if you are going to bald, and if you do, you may regret doing a forehead reduction surgery. When you are 25 and your pattern can be predicted through a Personalized Master Plan with a good hair doctor, then you should have a hair transplant hairline reduction which can accommodate hair loss without scarring at the hairline.
Thanks doctor. What is your opinion on how finasteride effects sperm, that’s really my main concern at the moment, I’ve read people saying their levels dropped to a point they would be considered infertile. Also if I was to start I would like to stay on for 10years max, I’m concerned fertility problems could be permanent after such a long duration.
Sperm counts often drop with finasteride so checking it before and after you are on it for a month or so will tell you how low it will get. My son, on finasteride for 15 years, saw a reduction a sperm count but he fathered two children, the second one was not planned.
There is no doubt that a hair transplant puts hair on the balding head and does it in a timely and predictable manner, in this case in just 5 months. I would expect that more length and possibly more hair is yet to grow in this man. If you are over 25, it is a very good option.


Telemedicine, companies in the USA (HIMS, KEEPS, ROMAN) send the 1mg generic to patients who fill out a form and submit it, no consultation with a doctor. They send either a 1 or 3 month supply for $20 to $30/ month. So patients are paying $240 to $360/yr for a product that often doesn’t work.
By law, only physicians are performing hair transplant surgery in the US and most European and Asian countries. Necrosis is a terrible complication of a hair transplant and necrosis reflects some lack of understanding of anesthesia and/or technique in the surgery. In the 16,000+ surgeries my group has done over the past 29 years, we never had a case of necrosis
![]()
I’m confused why people even consider FUE. FUT has clearly shown to be able to extract more follicles from the safe zone and have a higher survival rate. Our limiting factor is the number of hair follicles we have. So besides an unsightly scar (which we can wear our hair long to hide), why FUE over FUT?
For the men with advanced balding patterns like the Class 5-7 patterns, I personally believe that the strip surgery is better because you don’t develop a see-through donor area as the donor gets depleted with FUE when the number of total grafts extracted exceeds 3500 grafts. This applies to a man with medium weight hair and a normal donor density. Men with coarser hair and higher than normal donor densities can get more than 3500 grafts extracted safely with FUE
Does it? How does collagen help a hair cell which is dead in regrowing hair? I think it is the stemcell transfer that happens during the microneedling that help dormant cells to actually regrow back. Any thoughts?
Probably not if the area has really been bald for many many years. If it has been just a couple of years, some of the stem cells might be stimulated with microneedling plus minoxidil.
I red some people saying after hair transplant their scalp never felt the same again, like there is always some kind of weird feeling sort of numbness, is this a common thing? It’s said that since there is thousands of scars, it leaves small nerve damage
Some people get temporary numbness from the small nerve endings that goes away in a month or two at most; however, there are major nerves that the surgeon should stay away from which can give numbness to major parts of the head that can last years.
Those who have started taking finasteride before age 20, what have been your results?
The younger you are, the more likely you will see results. What we have seen is that when the hair loss is recent, finasteride is often more effective.
I have been struggling with hairloss since i was 21. When i turned 23, it was really bad. My temples were gone and it was very hard to hide it.
So i went to a private clinic in the Netherlands and they told me a 1500 FUE transplant would be good. But first i had to take finasteride. I was scared of finasteride, but i decided to take it. I’m taking it everyday since april 2019. And i had made an appointement for the transplant on 6 september 2019.
It has been almost 6 months since the transplant (5,5 months). It has been 10 months since i started taking finasteride. I actually started using dualgen 15 plus (topical minoxidil and topical finasteride) 2 months after taking oral finasteride. So i would say it has been 8 months since a started using this.
Overall i’m happy with the results. I think i’m maintaining my hair. There are periods where i lose a lot of hairs and there are periods where i lose a little.
Regarding the transplant, i wish my temples were denser. I know i’m still on month 6, but i don’t really see it getting better.
At 23, chasing hair transplants sets you up for a lifetime of doing it. Wait until you get more balding before you do another hair transplant. As a general rule I don’t do hair transplants on 23 year old men because the balding patterns are usually not evident and too much of the donor supply gets used up without a good Personalized Master Plan to be able to address your future needs.
I searched the sub but did not find an answer, sorry if it has already been asked.
I’m on the big 4 since the end of November. I know it’s too early to draw any conclusions but I already had very good results on top and front, managing to fill an area on the right temple that has been bald for 15 years!
However hair on the crown is still rather thin, as if it’s lagging behind. Does it take longer to regrow according to your experience?
My routine:
Finasteride 1 mg / day
Minoxidil 5% foam twice a day
Dermarolling 0.25 / 0.50 mm 3 times a week before applying Minox
DS Laboratories Revita shampoo 3-4 times a week (it contains ketoconazole, biotin, caffeine, etc.)
Biotin 5000 mcg / day
Vitamin D 5000 UI / day
The crown hair usually regrows faster than frontal hair with drugs like finasteride and/or minoxidil. I am not sure how the microneedling changes that. After a hair transplant, I believe that they grow at about the same rate.