Objective: The effects on scalp and serum dihydrotestosterone (DHT) of different doses of a novel topical solution of 0.25% finasteride (P-3074), a type 2 5?-reductase, were investigated in men with androgenetic alopecia. Methods: Two randomized, parallel-group studies were conducted. Study I: 18 men received 1 mL (2.275 mg) P-3074, applied to the scalp once a day (o.d.) or twice a day (b.i.d), or 1 mg oral tablet o.d. for 1 week. Study II: 32 men received P-3074 at the dose of 100 (0.2275 mg), 200 (0.455 mg), 300 (0.6285 mg), or 400 (0.91 mg) ?L or the vehicle o.d. for 1 week. Scalp and serum DHT and serum testosterone were evaluated at baseline and treatment end. Results: Change from baseline in scalp DHT was -70% for P-3074 o.d. and approx. -50% for P-3074 b.i.d. and the tablet. Serum DHT decreased by 60 – 70%. The doses of 100 and 200 ?L P-3074 resulted in a -47/-52% scalp DHT reduction, similar to the 300 and 400 ?L doses (i.e., -37/-54%). A -5.6% inhibition was observed for the vehicle. Serum DHT was reduced by only -24/-26% with 100 and 200 ?L P-3074 and by -44/-48% with 300 and 400 ?L P-3074. No relevant changes occurred for serum testosterone. Conclusions: The novel finasteride 0.25% solution applied o.d. at the doses of 100 and 200 ?L results in an appropriate inhibition of scalp DHT potentially minimizing the untoward sexual side-effects linked to a systemic DHT reduction.
I often tell my patients to check their sperm count before they start taking finasteride and then after a few months later if they plan on having children in the future. We know finasteride drops sperm count so it is something that men should know if they take this drug.
I don’t have the study done by Norwood and Shiell, but my memory is good that 7% of balding men (which is half of all men) will be a Class 7 by the age of 26. I suspect that the number for a Class 6 will be in the 15-25% range, but I don’t remember for sure. I did find this on the internet chart to point you to the age distribution for the Norwood Class 2-4 by age distribution to 40 years of age
This is a difficult question so i will try to guess relying on my 30 years in this business. Using a 70% probability (my opinion), by the age of 26 and using the HAIRCHECK instrument and trichoscopy you will know your final balding pattern, a 80% probability (my opinion), by the age of 30 and using the HAIRCHECK instrument and trichoscopy, you will know your final balding pattern, a 90-95% probability (my opinion), by the age of 35 and using the HAIRCHECK instrument and trichoscopy you will know your final balding pattern. A few men may be normal past 35 and still develop balding, but that may reflect less than 5% of men.
When I was around 14 my brother took me to the barber and made me get haircuts that looked good but required a hair dryer to maintain the look which I wasn’t good with. Every morning after having a shower I would use a shitty hair dryer on the max setting on my hair for a good few minutes to try and achieve the original look which I couldn’t really do and this went on for at least a year.
I thought I was balding since I could see my scalp when I looked close in the mirror but I wasn’t losing any hair and I was cutting my hair short so it didn’t really matter that much at the time but when I kept my hair longer it didn’t look pleasing so I decided to shave all my hair off because I thought it would remove all the “thin hairs” I had and then grow thicker hair which was all a waste.
That was two years ago and my hair is still weak and fine. How do I go about repairing my hair so it becomes thicker on the top? Should I use a Dermaroller?
Hair damage is solved as the new hair grows up from the scalp, while scalp damage to the growing hair follicles in the scalp can be permanent. See a doctor.
Hello Im balding as a 16 yo guy. My temples are already norwood 2 (but it doesnt matter as my hair covers it) BUT now recently I started shedding in the crown. When I brush my crown I find 5-7 hairs everytime. It didnt used to be so much a few months ago. And This is scary as fuck. But I dont know what to do. Should I start minoxidil? Please note that my crown balding isnt really visible yet and seems more like a cowlick, but this is terribly scary.
Im also concerned that minoxidil wont stop the shedding, will destroy my collagen and make me look older. Of course finasteride and other DHT related meds are out of the question here because of my age. What should I do?? Im really lost here, nobody believes me from my dermatologist to my family, they are all in denial.
Start off by getting a HAIRCHECK test ( https://baldingblog.com/haircheck-test-how-it-is-done-and-what-its-value/ ) to find out if you are really balding and then with a metric, you can follow the process over the years with yearly tests. As you treat the hair loss, you will know what is happening with the impact of the treatment.
The amount of brainfog i got from dutasteride is killing me I was using a pill a day for the last 15 months and i have brainfog… It didn’t go away for the last 15 days, am committing suicide? I am in my house with brainfog in my stupid dumb head quarantined…
Stop the drug! Those are bad side effects. See your doctor
The V-shaped hairline is the typical mature male hairline. I have written about hairlines here:https://newhair.com/wp-content/uploads/2018/11/phenotype-article-published.pdf which covers the different hairline shapes and how you get them as you get older. This link shows examples of both types of hairlines with some good photos: https://baldingblog.com/juvenile-vs-mature-hairline-am-i-going-bald-with-photos/
There doesn’t seem to be a consensus among studies with finasteride’s or dutasteride’s effect on women?
Premenopausal women should not take finasteride or dutasteride because if they became pregnant, the baby would have genital developmental problems. These drugs work in about half of post-menopausal women for hair loss.
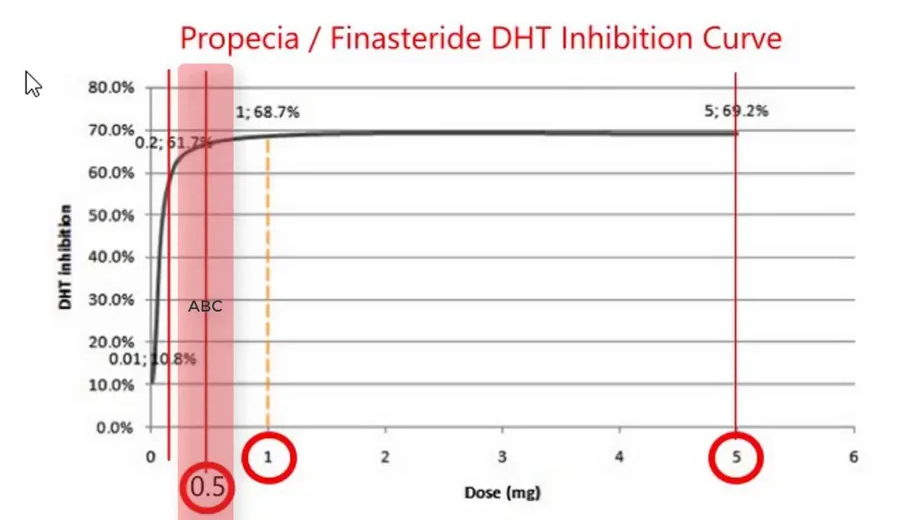
Just coming back to leave an anecdote of my experiences on fin, as I remember how useful I found these sorts of posts in the past. I’ve been on fin 2.5 years now. I was initially on the recommended dosage of 1mg until just before the 2 year mark sides started to appear in my life (loss of libido, morning wood, slight feeling of emotional numbness/dissociation). I decided to drop down to 0.5mg and it has honestly been the best move I could have imagined. A lot of posts that I read seemed to suggest that this would not make any difference but by god has it. Im now roughly 6 months on from changing dose and I feel virtually as I did pre fin.. and my hair is still going strong as ever (way way thicker than pre fin). If you change dose what I would say is just ‘patience’. It probably took around 3 months after changing for my body to ‘stabilize’ but I’m fairly certain now I’ve just found a dose that works for me.
Reducing the dose from 1mg to half the dose will decrease the effects by only 20% but you should work with your doctor on this plan. What is your Personalized Master Plan?
I grew out my hair a while ago and noticed way more hairs falling out in the shower and kinda freaked out too. It turned out that I was just noticing it more because it was longer 99% sure the answer is no, but wanted to ask just in case. I’ve been on finasteride for almost 10 years now and it’s worked really well, but around a month ago I decided to grow our my hair a little (it’s still pretty short, just longer than before) and I’ve noticed considerably more shedding when washing my hair, on the pillow etc. Is it just coincidence? Am I just noticing it more because it’s longer? Did anyone else experience actually more shedding with longer hair?
When hair is miniaturized, long miniaturized hairs are easier to pull out if you brush or comb roughly.
Dementia tied to hormone-blocking prostate cancer treatment
July 5, 2019 by Lindsey Tanner
Micrograph showing prostatic acinar adenocarcinoma (the most common form of prostate cancer) Credit: Wikipedia
Alzheimer’s disease may be a risk for older prostate cancer patients given hormone-blocking treatment, a large, U.S. government-funded analysis found.
Previous evidence has been mixed on whether the treatment might be linked with mental decline. But experts say the new results stand out because they’re from a respected national cancer database and the men were tracked for a long time—eight years on average.
Among 154,000 older patients, 13% who received hormone-blocking treatment developed Alzheimer’s, compared with 9% who had other treatment or chose no therapy, the study found.
The risk for dementia from strokes or other causes was higher: It was diagnosed in 22% of those who got hormone-blocking treatment, versus 16% of the other patients.
The results, using perhaps one of the largest and most reliable databases, suggests there truly may be a connection, said Dr. Sumanta Pal, a prostate cancer expert with the American Society of Clinical Oncology. Pal was not involved in the study.
The analysis from University of Pennsylvania researchers was published Friday in JAMA Network Open.
The results aren’t proof but experts say they underscore the importance of discussing potential risks and benefits when choosing cancer treatment.
The researchers analyzed data from a National Cancer Institute database of cancer cases and treatment and covers almost 30% of the U.S. population. The study focused on men in their 70s, on average, with local or advanced prostate cancer diagnosed between 1996 and 2003. They were followed until 2013. Medicare records indicated dementia or Alzheimer’s diagnosis.
Hormone-blocking treatment can include testes removal to reduce levels of testosterone, which fuels prostate cancer growth. But it more typically involves periodic drug injections or implants that achieve the same result.
Most U.S. men who receive this treatment are in their 70s or older. It’s sometimes used in men who might not be healthy enough to tolerate other cancer treatments including surgery to remove the prostate and radiation.
It’s unclear how the treatment might be linked with mental decline. The researchers noted that it can lead to diabetes, which also has been linked with dementia—perhaps because blood vessel damage from diabetes can restrict blood flow to the brain. Hormone treatment also raises risks for heart diseaseand depression, which both have been linked with dementia.
Researcher Grace Lu-Yao of the Sidney Kimmel Cancer Center in Philadelphia, said the potential dementia risks from hormone-blocking treatment may outweigh any benefit for younger, healthier patients with longer expected life spans.
While the study doesn’t prove that the treatment causes dementia, she said, it is important to tell patients “because of the potential impact of Alzheimer’s disease or dementia on the quality of life of patients and their family.” She was not involved in the study.
More information: Ravishankar Jayadevappa et al. Association Between Androgen Deprivation Therapy Use and Diagnosis of Dementia in Men With Prostate Cancer, JAMA Network Open (2019). DOI: 10.1001/jamanetworkopen.2019.6562
For the scientists in our group who are interested in how the drug works, finasteride is a competitive inhibitor to DHT and the effectiveness of this is shown in the graph below. Note that the inhibition works even at lower doses. The degree of inhibition at the AR receptor does not correlate directly with the effectiveness of the dose based on clinical finding; however it is nevertheless close to the degree of inhibition.
I’ve heard of new “DPI” hair transplants that are supposed to look even more natural. Does anybody have any opinions? I heard the biggest advantage is the density you can achieve with a low graft count. I just want to reconstruct my temples (I am 25 and they are just starting to go). If I could do this with only 500 or so grafts so I have more when I am older that would be fantastic.
DPI? When a new name is invented without a real new validated technology, it is a marketing ploy. There is no such thing as: ” advantage is the density you can achieve with a low graft count” other than to get your money. Use your brain and read my blogs at: https://baldingblog.com/ to educate yourself.