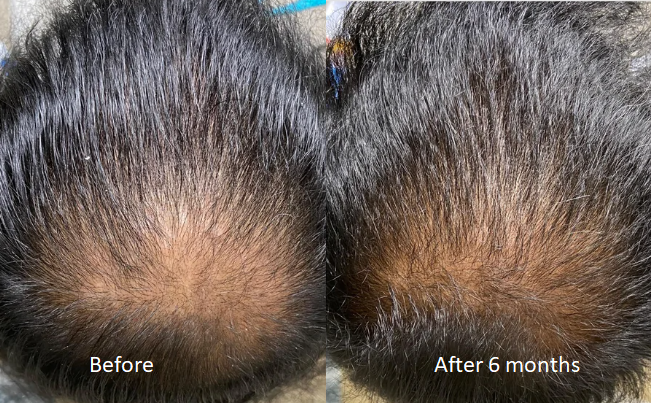
These photos show slow progress, with the hair filling in nicely. Give it another year and possibly a stronger dose and you might reverse the crown loss.
These photos show slow progress, with the hair filling in nicely. Give it another year and possibly a stronger dose and you might reverse the crown loss.
In elderly men, even those not afflicted with AGA, DUPA or ART, does the nature and quality of their hair still decline and get somewhat thin with age? Because most elderly men I’ve known, even if they still have all of their hair on their head, it doesn’t look like the same quality as it was in pictures when they were much younger or when they stand next to a younger person with all of their hair.
So I heard somewhere that when you do cardio blood flow goes to the scalp, and if you’re on minoxidil and you exercise it gives you faster or better results is that facts or myth?
This is a myth; however, exercise is always good for your health and as stress causes hair loss to accelerate, exercise destresses you to help you hold on to your hair.
I have been taking 1mg of finasteride daily for the past 3 years. About a month ago, I cut my dose in half to .5mg by breaking the tablets in half. After about 3 weeks of doing this, I noticed what appeared to be a higher amount of hair falling out when I would run my hands through my hair when wet (like after a shower). Could the drop in dose, produce more hair loss or is it a natural result of my genetic balding?
This man had 3300 grafts. Because he was blonde, the hair grafts needed were less as the color/contrast between hair and scalp color was closely approximated. He had some grafts placed in the top and crown, but most of the grafts were placed in the frontal area to give him an excellent frame for his face. He added Scalp Micro-pigmentation to make the back of his scalp look fuller. He accomplished his goal!

I’ve been reading about the history of hair transplants recently and I’m baffled by how in the 1950s, 60s, 70s, 80s and at least early 90s getting those awful plug procedures were the norm. I’ve also read that in Japan they started experimenting with hair transplant techniques in the 1930s and 40s, and one pioneer even mentioned that the grafts need to be small so they look natural. Did really nobody else figure this out for 50+ years and they thought walking around looking like having the hair of a doll was the best and most natural thing you could do?
That is the question I asked when I entered the business in 1991. I had observed the old technique in preparation for opening my own practice from 1990-1992. So, after watching the terrible deforming procedures that were the standard of care back then, I started on my first case to perform follicular unit transplantation in large quantities in a single session. The surgery was complex, and my first case was 700 grafts. Then I increased the next one to 900 grafts, then 1200 grafts, and well into my first 12 months, I could perform up to 2000 grafts per surgery. The size of my team increased significantly, with more doctors and a lot of surgical technicians whom we trained. By the second year, I got up to 3000 grafts and published the progression in the Hair Transplant Forum so doctors worldwide would understand the possibilities. Those old procedures produced many freaky-looking men, so I developed repair techniques that became the new standard of repair care in 1992.
In addition to publishing, I presented patients at meetings, starting in 1993 when I brought 3 patients to a meeting to demonstrate the results of this technique. In 1994, I brought 23 patients to the ISHRS meeting in Las Vegas, where hundreds of doctors were in the audience. My presentation required a long break after, as the patients were viewed firsthand, outside of the conference room. That set a new standard until 2002 when I pioneered the FUE procedure after a 6-year development process. I brought one patient to the conference to show off the results, as well. Everything I did, I published in top medical journals. Young men who understood what I had done started demanding it from their doctors, who eventually either quit practicing (because it was a long, complicated, and tedious procedure) or adapted. I still practice that art form today, with the FUE I pioneered in 2002.
My hair has been thinning for the past 4 to 5 years. I started taking 1.25mg Minoxidil daily and 1.25mg of Finasteride three times per week about 7 months and I can already see that the meds are working. In terms of the current state of my hair, I still have a pretty decent hairline. The issue is that my hair is thin in the crown, mid-scalp region and frontal region. Its thinnest in the crown. I don’t think I’m ready for a hair transplant yet. Like I said my hairline is decent and I would like to keep that natural looking hairline for as long as possible, and I’m confident I can now that I can see the meds are working.
But to help with the areas that my hair is thin, I’m considering getting scalp micropigmentation (SMP) to give my hair a more fuller appearance. I was just wondering has anyone here had smp done (without getting a hair transplant)? And I don’t mean on shaved head to give the appearance of stubble all over. I mean getting smp done as a way of making an existing head of hair appear thicker. If anyone has had something like this done, how were the results?
As the doctor who wrote most of the articles in the medical literature on Scalp Micropigmentation, I wouldn’t rush to do it. Most people who do SMP, do it poorly, and a bad job is worse than no SMP at all. If you decide to do it, make sure that you see a couple of patients that were done by that provider. Give your medications a chance to work before going to SMP.
Does your hair change colour or look lighter if your a diffuse thinner? Eg going from black to brown?
Does shedding actually indicate balding?
Does a diffuse thinner end up NW6/7
Great result, which shows the sensitivity to crown hairs to these two drugs.

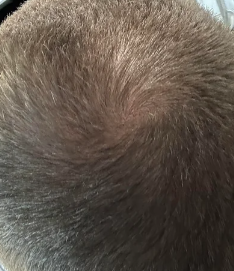
Yes, you appear to be growing new hair where the arrow points. Is appears to be early growth and in time it may get better

Our body has feedback loops. Possibly your body recognized the need for more testosterone production which would raise the DHT levels. This could explain the many men who told me that their sex drive went up on finasteride. In the future, for these men, I will offer DHT blood testing for these men with increased sex drive on finasteride.
Is fut better if somebody is willing to do multiple surgeries throughout their life? Or is fut preferable in that case? Thanks.
It makes no difference for lifetime hair transplants if you go to FUE or FUT
I have been taking finasteride for 3 years and it has helped me a lot in stopping my hair loss. However, after my last check, it turned out that my Testosterone (from 24.82nmol/l to 40.79nmol/l) and free testosterone (443.6pmol/l to 821.9pmol/l) have increased since my last check. My doctor has advised me to come off finasteride for 4 months until my next check up, although I suspect that such a period of time will definitely ruin my hair again. I know I did strength training the night before the blood test, is it possible that it raised the test levels that high? I don’t want to go off it for that long when I know it works great for me.
Testosterone levels often rise when taking finasteride. Stopping finasteride for 4 months may be a disaster for your hair as hair loss is almost a certainty if you have had significant benefits from taking the finasteride (these benefits will reverse). I don’t believe that your doctor understands the drug finasteride, and he/she needs to get educated about it.
Can pulling dandruff scabs cause permanent traction alopecia?
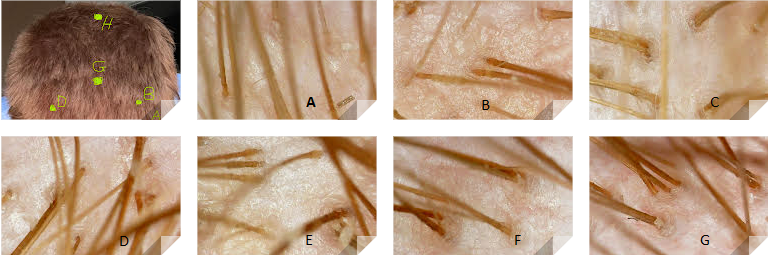
This is a 26 year/old male who was concerned about balding, especially recession in the two corners of his hairline. This man has a very large and strong forelock. It takes over a good 70-80% of his hairline, and in the center, it is located where it was when he was 10 years old. Many men with strong forelocks, even if they are bald behind them, will maintain an excellent frontal hairline look. In his case, the two corners are developing their mature position, making it look like he has corner recession, which he does not. To be sure that he was not balding either in the forelock or the corners, or even behind the forelock, he purchased a hand microscope from Amazon and then took these pictures, mapping out the microscopic photos to the photo of his head. As you can clearly see, there is no miniaturization anywhere on his scalp