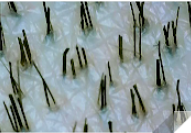
This is an excellent photo showing that you have a very high donor density of about 2.7 hairs/follicular unit. The normal Caucasian person has a donor density of 2.2.
This is an excellent photo showing that you have a very high donor density of about 2.7 hairs/follicular unit. The normal Caucasian person has a donor density of 2.2.
Some doctors are so orderly that they line up hair grafts like toy soldiers when they do a hair transplant. Sometimes these patterns show in the final result. Here are two photos 2 days (on the right) and 2 weeks (on the left) from the date of his hair transplant. He is rightfully concerned. Since I posted this photo, I was given new photos of him at 5 months growth. The hair that lined up at the time of the surgery, can be seen now when you look at him. He wants me to fix it, an easy fix as I have done thousands of these. I advised him to wait until he is 8 months out before undergoing a repair surgery with me.


Good morning, I came across your balding blog and think that it’s a great resource. Thank you for doing that. I see people ask you all sorts of questions and I wasn’t sure how to post on there and/or ask something anonymously so I figured I would email you. I had alopecia on my scalp into which I had roughly 3,200 FUE grafts transplanted into the scar to conceal it (not all at once but in smaller separate procedures). I uploaded a picture of about a centimeter or so of my donor area where grafts were extracted and was wondering if you can from the picture help me estimate roughly how many grafts I still have left in my donor in case I want future transplants. I counted 32 follicular units and 78 hairs so that comes out to an average of about 2.4 hairs per unit. I tried doing the math I saw you explain on one of your threads and here is what I got. The average donor area is 12,500 units X 2.4 hairs = 30,000 hairs. You need roughly 12,500 hairs remaining in the donor area to provide adequate coverage so 30,000-12,500= 17,500 movable hairs. 17,500 hairs ÷ 2.4 hairs per graft equals 7,291 available grafts that I could move. That would have meant that before I used those 3,200 grafts for the scaring alopecia that I would have had a total of 10,491 harvestable grafts in my donor. Is that even possible?
Your donor density is higher than average. What you didn’t take into account is your hair thickness, a very important factor in determining your harvestable donor area. Remember, that there are only 50,000 follicular units on the head of which 20-25% of them are in the donor area. If you are thinking that you take out more than half or 2/3rds of your donor area hairs, you will be in trouble if you have fine hair, which I believe is your situation.
How many grafts were removed totally? Answer 3200. Were these all follicular unit grafts? Yes? Subtract that number from 12,500 total donor supply and the remaining follicular units and you get 9,200 graft remaining. If your hair is fine, the actual number of grafts that are available will be significantly less than if your have a coarse hair. Medium is somewhere in the middle. You might still have a significant donor reserve based upon the hair thickness of the donor hair provided that you hair isn’t fine as I suspect it is. Does this help?
This patient had some small benefits in the bridge hair in the middle of his head, but most of the real benefits were in the crown, which clearly grew new hair. The frontal area did not respond to the microneeding, which is not unusual with long-term balding.


1) In a previous email, you stated that you’ve removed a strip of skin/scar from elsewhere on the scalp aside from the usual donor area and extracted grafts from it; we had been talking about the temporal region since I had a scar there with grafts placed into it. Strips that are removed from the temporal region, do they typically heal well with minimal scaring?2) If grafts from a second procedure were placed on top of grafts that have yet to surface from a previous procedure, what will happen?3) People with diffuse patterned alopecia, do they eventually lose all the hair in the areas that they are thinning and end up with a slick bald scalp? Or does the hair remain but just is thin?
Treating your badling with standard medications like finasteride and minoxidil and sticking to it get excellent results in many men without needing a hair transplant.

Any concern in SMP while on topical min fin? And what about a transplant with SMP on scalp?
Once the SMP is set (about 1 -2 weeks), the use of minoxidil is not a problem. if you had SMP and wanted a hair transplant, there should be no problem as any good surgeon should be able to work with SMP present.
Amazing, as this looks like full reversal of his recession.


Amazing that microneedling can regrow the hair in the crown in just 6 months. Congrats! The question we don’t know the answer to is, “What happens to the new hair when the microneedling stops?”


Amazing rapid growth. I suspect that you will see much more hair over the next few months.

If you develop hypertrichosis from minoxidil, stopping it will cause all of the minoxidil-grown hair to fall out. This may take a few weeks or even more than a month
If someone has a hair transplant procedure and 6-8 months later they have an additional transplant procedure, since it can take up to a year for all of the transplanted hairs to surface, what if in the 2nd procedure they place a graft in the same spot as a graft that has not grown yet from the 1st procedure?
Actually, by 8 months, 99% of the grafts that are growing have broken through the skin. Some telogen hairs may break through later on, but this is not a significant amount.
I am surprised that this man actually got some reasonable results from microneedling in what we refer to as Atrophic scalp, that is, a person’s scalp that hasn’t had hair for, in his case, 14 years. He used minoxidil and finasteride as well. This man got a response in just 3 months indicating that the stem cells are still viable.


What is the effect of minoxidil to the hair follicle? How can you tune the dosage to manifest the effects on hair?
I fear I may have developed DUPA. My sides and back have become transparent and I am approaching an NW7. I have added oral fin, oral min, and topical pyrilutamide which I believe has helped and the oral min has regrown some hair and increased thickness a bit. But the density is still poor. I still experience some itching and tingling along my hair line, even for my beard which is patchy. I am wondering if there are natural anti-inflammatory treatments I can add to my regimen to combat loss from inflammation. Is there a such thing as a natural JAK inhibitor that may be gentle enough to help my DUPA?
I have read that for DUPA sufferers, inflammation is the cause of hair loss, where the immune system attacks all the hair follicles of the head. This seems relevant to me because right after a shower if I have scrubbed and dried my skin a lot, I notice a lot of puffiness, redness all over and tingling and itching and hair fall from my scalp and even beard. So I fear inflammation is attacking my hair. I have also suffered skin conditions like eczema resulting from inflammation in the past. I am afraid to try JAK inhibiting drugs to combat inflammation because they come with high risk of potentially deadly sides.
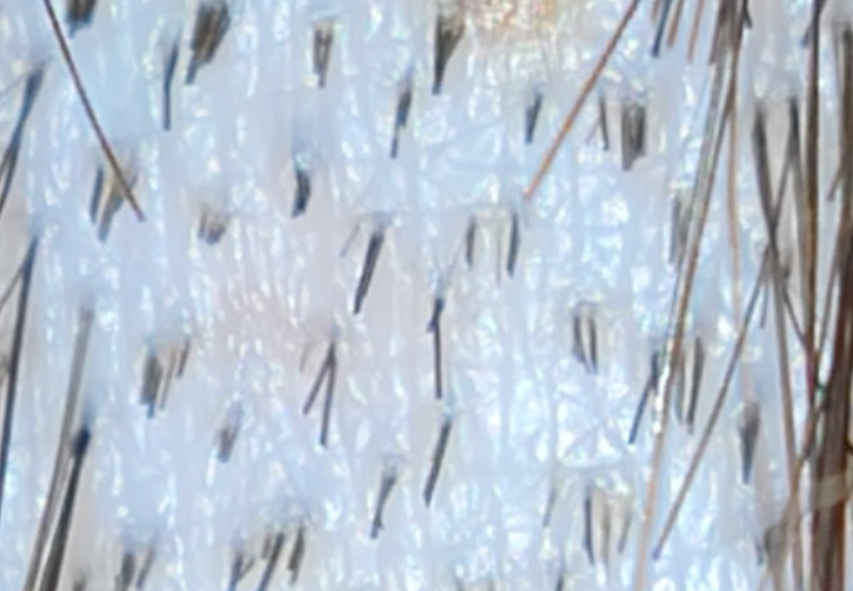
Your discussion was interesting to read. Please make sure that you have DUPA. This is what it looks like, so get a hand microscope and see if this is what you have: https://baldingblog.com/classic-case-of-dupa/