Yesterday, we did SMP (Scalp Micpigmentation) on a patient whose hair transplant didn’t quite achieve the desired FULLNESS he nor I wanted to achieve. He reached his limit of grafts at about 4000 grafts but still wanted a full head of hair. He had a very large head and a poor donor density. I subsidized his 4000 donor area grafts with 500 beard grafts to the crown in the second of two procedures. This gave him just about enough hair to lightly cover the crown. With SMP, his situation has changed radically, as you can see with the before and after photos taken 4 hours into the SMP, which was still going as this post was written.
This is a wonderful approach when hair fullness (notice I didn’t use the term density) is not achieved. Density is just one element that contributes to the LOOK OF FULLNESS. Other aspects contributing to fullness include the color/contrast between hair and skin color (SMP addresses this very nicely, as shown in this photo below), the thickness of each hair follicle (this man had fine hair reflecting poor hair bulk), and the needs of the balding area (can be expressed in square inches of balding area compared to the donor supply). This man has a Class 7 balding pattern, where a 4:1 imbalance exists between the size of the bald area and the donor area (in his situation, less than half can be used). There is clearly a limit when the graft supply is exhausted.
The patient and I discussed this before the very first procedure, and he went into this with his eyes open because I developed a Personalized Master Plan for him as I started his reconstruction. His first procedure was designed to build a hairline and put enough hair in the frontal 5-6 inches to frame his face and give him some light top coverage. The transplant brought the coverage to mid-scalp. He had a fantastic result and he styled his hair to take advantage of combing it from left to right. The second procedure took it further back to the top and crown. I used beard hair mixed with some scalp hair for this area. In this last procedure 1 year ago, I included some beard hair for his bald crown. When all of this grew in, the back of his head was sparsely covered but with enough hair that a comb-over would suffice. The SMP is the topping to this process as it created the fullness that he desired.
I published an article in 2018 in the Journal of Plastic and Reconstructive Surgery on this philosophy. The theme of this article was that when combining FUE and SMP, the surgeon can almost transplant any healthy man, provided that the donor area is healthy. As this article has been read more often since it was initially published (I receive tracking of the reads), more and more surgeons are adopting this approach in planning a hair reconstruction on men with lower-than-ideal donor densities, fine hair, and advanced balding patterns. This approach requires an excellent team to back up the surgery, including perfection on the SMP side of the equation, as shown in the photo below.
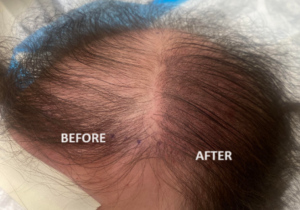 This photo was taken when only half of the head was done in the mid-point of the procedure.
This photo was taken when only half of the head was done in the mid-point of the procedure.