Is hair miniaturization always male pattern baldness?
Mostly miniaturization indicates hair loss is probably genetic in both men and women.
Is hair miniaturization always male pattern baldness?
Mostly miniaturization indicates hair loss is probably genetic in both men and women.
Is it better to do it sooner or does it really matter when you undergo surgery? do I need to rush into it or will the results be the same if I wait a couple of years?
Timing of the surgery is a personal decision. The question is if you are bald, can you handle it, or , if you are becoming balder, can you handle it? If you are over 25, a hair transplant can be an option. Will getting your hair back now make a difference in your life?
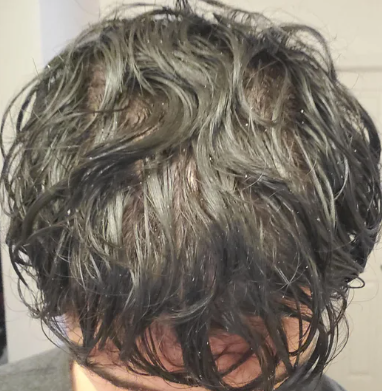
Some nice early new hair can be seen in the crown area with more filling present. Give it more time and the picture show will become more and more evident

I don’t know if I am just super conscious but I started to lift again about 6 weeks ago and it seems like there is much more hair in the shower falling out than before, isn’t it true that lifting will release more DHT or something? or am I just panicking
Wight lifting without taking any medications or supplements, will not cause an increase in hair loss. In fact, it may reduce enough of your stress to take the stress off of the hair loss.
This photo shows that minoxidil alone can reverse hair loss and cause new hair growth in the frontal hairline. Some of the growth appears recent with early corner filling

Yes, both can simultaneously. That means that if you have DUPA, you should never have a hair transplant because the grafts will eventually fail sooner than later.
To find out if you are really losing hair, get a HAIRCHECK test (https://baldingblog.com/haircheck-test-how-it-is-done-video/ ) and this will actually measure the loss and then you can follow what happens over time with treatment.
I took finasteride for almost 30 days exactly around june last summer, but quit due to noticing gyno coming on, once i hopped off the gyno has stopped progressing but i still have a slightly watery semen and just last week i started having ball ache, it started very mild but it’s just been getting worse and worse. i’m going to try to get recommended to a hormone specialist or something on monday. has anyone else had a new side effect come on this late after stopping fin use? should i be very worried or is this just something minor? i haven’t had any ed problems or libido problems that i can notice, but i’m afraid that’s next
There are many causes of testicular pain and if you are off finasteride for 7 months, it is likely that you have one of these other causes. See your family doctor
We continue to see over-harvested donor areas where those doing the hair transplants take out so much donor hair that they start making the donor area bald. In this man, clearly the hair transplants also failed as you can see from the top of his head. The donor hairs were also taken from his neck area which is not permanent hair.
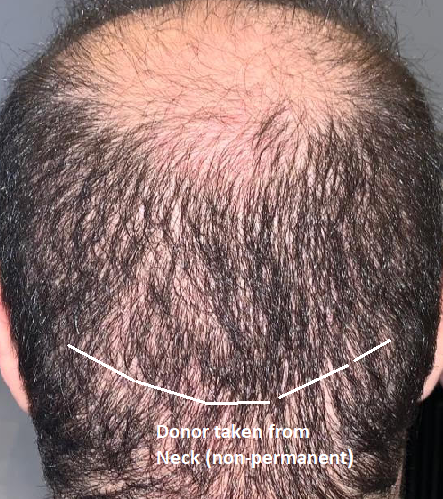
Click to enlarge
If you are losing hair, you should meet with a good doctor and develop a Personalized Master Plan for your long term hair loss problem and its treatment. Be strategic and don’t mess with being your own doctor. There are good drugs for you that work very effectively such as finasteride and minoxidil.
Almost all of the grafts collected by this surgical team was either transected or mutilated. It was surprising that the team was proud of them enough to publish this photo. Significantly less than half of these hair will survive the transplant. Is this a brargain?

PFS patients often don’t follow up with their original doctors (as was the case here). There’s not much of a point really other than to inform the doctor what happened. Sometimes they do and the original doctors downplay the situation, tell the patient it will go away, and when it doesn’t they don’t bother following up. The doctor will often assume the problem went away even though it didn’t. Even worse they say the problems weren’t caused by finasteride and they should seek help from a specialist. Here are just some of the dynamics that play out when patients get PFS. It is getting better now that people are more aware but it is taking far too long and it is all because Merck lied to doctors, the public, and maybe the FDA over 20 years ago.
I never followed up with my original doctor beyond an initial email because he didn’t know any more than what was on the product label. This was over a decade and he probably thinks I’ve recovered. Merck’s warning label basically encouraged doctors to keep patients on the drug because it said side effects discontinued in “most” cases for men who continued the drug and “men who discontinued”. They just lead you to believe it was “all men”.
I make sure to bond with my patients. For example, I will often spend 30-60 minutes with each patient who comes in and it is always free. That establishes a bond between doctor/patient and I believe almost every patient follows up with me because they know that I listen to them.
Be straight out about it. If you can’t, consider Scalp Micropigmentation which solves the problem ( https://scalpmicropigmentation.com/ ).
How old are you? There appears to be some early miniaturized hair along the right hairline and the corner seems to be going upward. Without a full view of your hairline with your eyebrows lifted high so that the forehead creases can be seen, I can’t help much more.

I’m a 22 year old male with androgenic alopecia and diffuse thinning. I’ve been balding since I was 18 years old.
Recently, I’ve been experiencing very rapid shedding all over my scalp (top of the scalp, donor area, and both sides of the head). I went to my dermatologist and had a scalp biopsy (4mm, punch) done to make sure it wasn’t alopecia areata. Turns out, it’s telogen effluvium due to various stressors. 12 days later, I got the stitches removed from the area.
BUT
The hair that is currently growing out and closely around the biopsy site are probably the thickest that they have been in YEARS.
I currently use a topical minoxidil 7%, finasteride 0.1% compound solution ((been using for 1 month), stopped taking finasteride tablets due to sides (used for 2 months)) and I use a microneedling pen (1mm, once per month). Although I’ve had very subtle hair regrowth on my hairline and slight thickening on my temples, the hair from the biopsy site feels and looks thicker than most of the hair on my scalp at the moment.
I’m aware that it may seem like an “illusion” due to my current TE condition, but it honestly feels much more thicker than before the initial shedding started. It almost nearly resembles the texture that it was from when I was a teenager.
If anyone is familiar with the biological components of hair loss and hair regrowth, I would love to hear from you about this matter.
Wounds sometime stimulate hair growth much like microneedling does