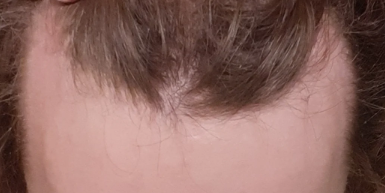
Pictures tell the story! This type of change is unusual in men over 25.


Pictures tell the story! This type of change is unusual in men over 25.
You appeared to have reversed most of your corner recession and the hairline looks more solid. Congrats!


So I just finished my procedure 2 days ago and just today went in for my final kinda checkup. I always thought that after the transplant you would still have to use fin and mono but my doctor said otherwise. He told me that men generally stop losing hair at the age of 28-35 and after that all the hair you have will stay basically forever.
[If you have any questions, you can reach me at williamrassman33@gmail.com]
Hair loss is progressive throughout your lifetime (assuming you have genetic balding). Generally, most hair loss occurs in men before they are 30; however, fewer men will start losing their hair in their 30s, 40s, and, much less frequently, in their 50s. Drugs like finasteride, assuming you can tolerate it, are lifetime commitments. I have had patients on these drugs into their 50s and 60s, and a few stopped them, regretting the hair loss that followed. Oral minoxidil may be similar to finasteride in its long-term value; however, good, long-term documentation is not available for minoxidil. After a hair transplant, your native hair is subject to progressive hair loss. Those who had a hair transplant and took finasteride probably noticed that they didn’t develop post-op shock loss because finasteride protects against it. For those of you who had a hair transplant, I am sure I would hear horror stories of shock loss from their native hair because their doctors were not proactive in preventing this often devastating condition.
Note that his donor area hair is not high in the back of his head, and much of the donor area we can see is see-through. This man, fortunately, never had a hair transplant for it would make his situation worse and it would produce significant scars, adding to his problem.
[If you have any questions, you can reach me at williamrassman33@gmail.com]

You have a tighter hairline, and the corner recession appears to have reversed.

I’m using the Dr. pen ultima A6 pen on my hairline which came with 36 pin cartridges. Is 36 pins good, or is something like 12 or 42 better?
The crown loss reverses easily with finasteride. The frontal reversal may be best by adding the combination of the two approaches, including oral minoxidil plus microneedling.

A couple of weeks ago, I started on Fin 0,25mg daily but have no clue if this will get me results and how fast compared to 1 mg. What is your advice?
I am NW2 and my dermatologist recomended I do PRP after I told her I would not take finasteride. She told me PRP is promising for me since I am relatively young and still have most of my hair. She said PRP is a better hairloss prevention than regrowth method and it would probably keep my balding from getting worse which is more than good enough for me considering I had already come to terms with the fact I will be bald. I don’t care about growing back my hair I’d rather not lose more without subjecting myself to anti androgens if that is a possibility. If it comes down to it I will go bald before I risk my health though. After hearing that PRP might actually save me I was thrilled and filled with hope that I may be able to save my hair without taking drugs. Then my derm sprung it on me that they charge $500-$800 per session. I thought for sure I could find someone to do it cheaper so I called around every doctor office and medical office with 200 miles of my city and every single one charges a minimum $500 per session which is ridiculous considering prp is a relatively easy procedure.
I don’t have that kind of money especially not for something that might not even work.After doing research on it I have decided to buy the equipment and do it myself. You can buy all the equipment needed for less than $500. I also wanna point out that I am a seasoned EMT so I have some medical experience and I’m used to working in less than ideal conditions. So I have bought a centrifuge and all the needles and vials needed to make the prp the one thing that really bothers me is I could not buy the fda approved PRP vials since I don’t have a medical license to buy them so I instead bought prp vials from eBay but who knows how sanitary they actually are I’m almost certain they are from China. It is because of this concern that I am not really comfortable injecting myself with this PRP but I don’t see any harm in microneedling with it I already have been microneedling with oils and hyralaunix acid so my question to anyone with experience is can I effectively fend off the reaper with a PRP and a .75mm dermaroller? I have all the equipment and I am willing to do it as frequently as possible.
Do you know how crazy it is to buy some concoction from eBay, not knowing its source or its sterility? This could be dangerous stuff you would be injecting into your body! I’m not a big fan of PRP as there is no consistent standard on how it is used. I have not seen good, consistent results from PRP in anyone’s hands. The microneeding is the benefit, and considering the costs you outlined above and the risks you might be taking, microneedling yourself is a very small cost by comparison; the proper depth for microneedling is 1.25mm. That will allow the needles to reach the stem cells. The Dr. Pen microneedling device, held for 10 seconds in each area, delivers a known injury that will start the healing cascade that leads to stem cell activation and reversal of hair loss in many men. If you really have a Norwood Class 2 pattern of balding, then why are you doing anything as the Class 2 pattern is not balding, but reflective a mature hairine? You might send me photos at williamrassman33@gmail and I will tell you if you are balding at all.
[If you have any questions, you can reach me at williamrassman33@gmail.com]
In just two months, this 27-year-old man reversed most of his crown loss. I have little doubt that the microneedling depth of 1.5mm, with weekly frequency, accelerated the return of his hair.


Web MD wrote a detailed article about shampoos, their ingredients, and how these ingredients help or harm your hair. I summarized today’s article as relevant to my readership and added some comments that I thought may shed more insights into the content. The most important takeaway here is to be careful about claims as to what any particular shampoo will do for you. If you look at the ingredients on the shampoo label, you will see the items discussed below. Educate yourself, especially if you have particular hair problems. Everyone reading this should know that the hair grown from the head is not alive once it appears from the scalp; it is dead tissue like your fingernails. We want to do things for hair to make it look and feel better, fuller, and more vibrant, but we certainly can’t give it life.
[If you have any questions, you can reach me at williamrassman33@gmail.com]
The Bombay High Court is seeking action against a dentist performing Aesthetic and Hair Transplant Surgeries as a result of a public interest litigation petition. The dentist was trained as an oral and maxillofacial surgeon, apparently under the auspices of his Dental license. The action is being taken because the Dental Council of India filed for permission for oral and maxillofacial surgeons to perform this type of surgery.
The demand for hair transplants has made this field lucrative for many doctors ever since the FUE was introduced as a clinical alternative for strip hair transplant surgery in 2002. The FUE has gone viral as a surgical procedure, as the learning curve is compressed for the surgeon who hires skilled available technicians. This had extended to Turkey, where over 1 million hair transplants were being performed by non-licensed technicians (who learned the technique by watching doctors or other technicians) until just recently. The Turkish government appears to have cracked down on these non-licensed clinics.
Please note that hair transplant surgery does not JUST require FUE skills. It requires many other skills, so be careful when checking out doctors who offer FUE without credentials or training. Deaths have occurred because many of these “Black Market Providers” don’t understand the effects of even something as simple as Xylocaine and the long-acting Marcaine, commonly used in dental and other cosmetic practices. Too much Marcaine will paralyze the heart, while too much Xylocaine will cause seizures, possibly leading to asphyxiation.
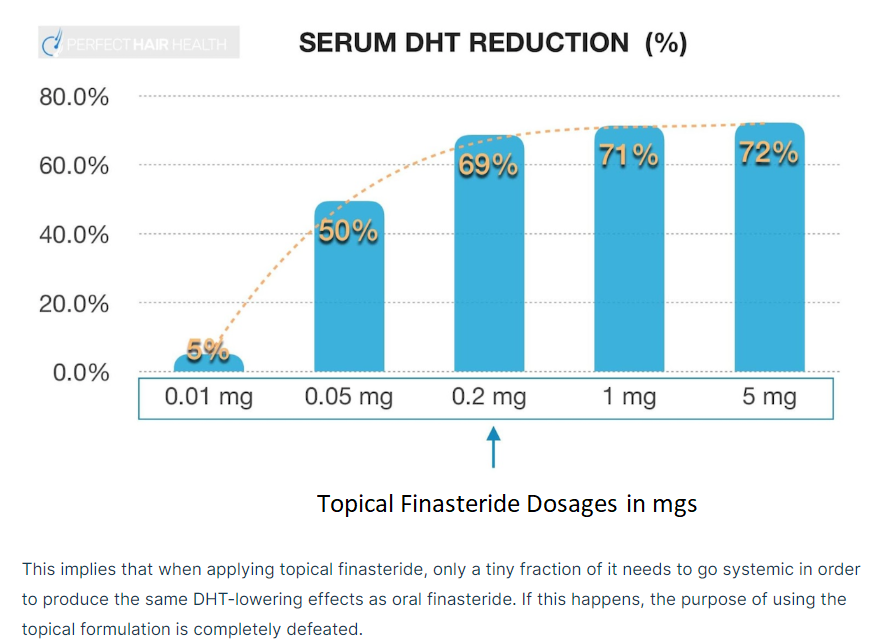
I was wondering if using a derma roller increases the probability of excessive absorption of topical finasteride, and thus the risks of averse reactions? If yes, what would be a good strategy to avoid this? For example, could someone simply not use topical finasteride on the day they use the derma roller? But since the effects of the derma roller last for more than one day, wouldn’t the risk of increased averse reactions from topical finasteride still be present in the following days?
Click to Enlarge