Yes, minoxidil has known side effects, and one of them is dangerous. It is called Pericardial Effusion, which means fluid builds up inside the heart sac. As the fluid builds up, blood is restricted from entering the heart. This produces significant swelling of the legs and feet, shortness of breath, and easy fatigue, and if it goes untreated, it could kill you. If you note swelling of your face, hands or feet, notify your doctor and consider stopping the minoxidil. It is also a hypotensive agent, and some men can’t tolerate it because of fast heartbeats and repeated bouts of headedness.
To answer that question accurately, I would want to see (1) a photo with your eyebrows lifted high so that the creases on your forehead show with your hair pulled back, (2) a measurement with a micrometer of the thickness of your hair shafts in the back of your head and (3) I would like to see a hand microscope view of your donor area with the hairs cut short (see here: https://baldingblog.com/creating-a-personalized-master-plan-for-present-and-future-balding-photos/). If you want my opinion, then you need to work this out between us by emailing me at williamrassman33@gmail.com). I’ll show you how to get the measurements and then let you know what you need. The goal is to determine the value of each hair in the donor area and the quantity of “lifetime’ hairs in the donor area, then calculate what can be achieved and match it against your expectations to make sure that they are realistic about number of grafts and defining the expectation after a single hair transplant.

As a man, I don’t know what you are talking about. I have never felt my prostate in any manner. If you are talking about orgasm, then yes, I have heard that finasteride, in some men, will reduce the volume and consistency of the ejaculate, and that may decrease the pleasure of orgasm for some men. I had taken finasteride for many years and never felt that my orgasms were any different than when I was not on finasteride.
Finasteride is more effective against the crown than elsewhere on your scalp. The photo shows that the hair loss starts above the swirl and moves to the frontal area. It is worth a try using finasteride, but if you use it, stay the course. Usually, the crown is more responsive to finasteride at any age than the frontal hairline.

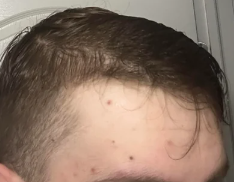
I’m mid 40s and have Been on Fin for year exactly now. Hairline has definitely seen an improvement but after getting a haircut yesterday I am now wondering if the temples have improved a bit too. Here is a comparison between July (pic on left) and Dec (pic on right). Is it just me or is the temple hair coming forward a bit?
The temple peeks do not have the same genetics as the balding scalp. What you are pointing to may or may not be regrowth. This would be unusual from finasteride which doesn’t seem to implact the temple peaks in my experience.

I have been using topical fin/min for about a year with fantastic results, but haven’t noticed my hairline improving. I’m wondering if microneedling will help, and have done some research that suggests it will. I’m confused about a few things: – I’ve seen people mention .3mm daily and .5mm once a week. But the Dr. Pen dermapens I’m looking at don’t seem to specify size. How does this work? – Can I microneedle and use topical fin/min at the same time? I believe I can, but I want to be sure
Microneedling might bring back the frontal hairline. It is worth trying. Best, after doing the microneedling, hold off on the topical minoxidil and finasteride for at least an hour.
I have seen changes in hair character on occasion. One man that I remember well, his hair changed to kinky. He loved it. I did a second transplant on him, and the same thing happened. Since this is rare, something in the patient must have caused this change. Seeing changes in your hair, from straight to wavy, is often a good thing as it improves coverage.
Hi, I’m currently 22 days post op and I’m not not sure if my hair looks right? The newly transplanted hair looks much thinner than the rest, I know I may have experienced minor shedding but does it look normal for this stage?
Yes, it looks fine. The grafts will likely shed in the next week or so, but don’t worry, as the stem cells remain to regrow the hair between 2-5 months from now.

Results like this are seen in men under 25. The older you get, the less likely you will get results like this.

I was shocked at the scarring I got from the FUE. Nobody told me that this was a risk. I am going to grow my hair right back to hide this scarring.
In surgery, we call this “Informed Consent” that your surgeon must always warn you of all of the risks of the surgery you are going to have. This is the law in all 50 states in the US as well as most Western countries.

This man had two sessions of grafts, 7000 and 5000. Most of the grafts clearly did not take. Assuming that all follicular units are excised in the donor area, the total donor supply equals 25% of the total hair supply. The average man has 50,000 follicular units (grafts) on his head, of which 12,500 reflect the donor area (12,5o0 is 25% of the total follicular units). This means that if the surgeons did only FUE, nothing would be left in the donor area (maybe 500 or so). In such a surgery, the patient will likely become either bald in the donor area or heavily overharvested in the donor area if partial follicular units are excised.
There is a misconception that many patients and surgeons must replace the recipient area density. Nothing could be further from the truth. First, look at the above numbers. Assuming that a patient has a Class 7 balding pattern, he is only left with his donor area remaining, which contains 12,500 grafts. A Class 7 balding area contains 37,500 Follicular Units (grafts). If all of the grafts in the donor area (12,500) were moved to the entire bald scalp and 100% of the grafts grew, then the patient would have achieved only 33% of their original recipient area density and become bald in the donor area. This is simply mathematics. So, transplanting into the recipient area should not blindly remove as many grafts as possible and move them into the recipient area. A surgeon, with proper knowledge of both the original donor density and hair mass of the patient’s donor area, can make appropriate artistic and mathematical calculations to obtain good results with less than the original recipient area density achieved. I have done this thousands of times on very bald men, even those with a Class 6 or 7 pattern of balding, and never removed 12,5000 grafts over the 33 years I have donr hair restoration surgery.
FYI: 50% of recipient area density in a man with black hair and white skin is as good as 100% recipient area density. This was demonstrated by Dr. Manny Marrit some years ago when he plucked out 50% of the hairs on one side of the head of a man with medium-weight hair, which was black, and his skin was white. No one could tell the plucked side from the on-pucked side.
This man needs an expert hair transplant surgeon to figure out what was done and how to give him a satisfactory appearance, if possible. This is something I have done a thousand times or more.
This photograph reflects that whoever did this transplant had a sense of order, so the grafts were lined up like soldiers in a straight line. Still worse was the straight-line hairline. If this man has straight hair, he will see the line-up of the hairs, but regardless of his hair characteristics, the hairline is so straight that anyone looking at it will know it is transplanted once it has grow out.

This 59-year-old male has had multiple hair transplants with me as he progressively lost his hair over many years. The last transplant was in 2019. He would have had a Full Norwood Class 6 balding pattern, but he kept the hair on his head with diligent medications and strategic transplants following a Personalized Master Plan he and I set up at the onset of his balding. When I did the last transplant a few years ago, I suggested that he get Scalp Micropigmentation (SMP) for his hair rather than get another transplant. He worked outside the United States for an oil company, so scheduling was difficult. Finally, one month ago, he came in to see me specifically to get SMP done. His hair is straight, as you can see in the frontal view, so straight hair draws the eye to the scalp, making it hard to use various styling techniques to cover the see-through nature of his straight hair. He could have grown the hair longer, but he didn’t want to do that. Now, with the SMP, I believe that he is finished with his reconstruction. He maintains himself on finasteride daily without side effects. The after photos are in the second row. I always talk about the value of SMP in men or women with see-through hair transplants or thinning hair as a great adjunct to their reconstruction, as shown nicely in this man. I would like to call your attention to his frontal hairline. It is not as straight as a line, as I built a transition zone between the thick hair and the forehead using 400 single hair grafts in a random placement when I reconstructed his hairline.

AFTER SMP Photos below:


There is little doubt that the microneedling reversed this Norwood Class 7 balding pattern. As for hair cycles, I wonder if he didn’t maintain some microneedling routine and if the new hair will stick around. I believe that microneedling should be maintained at least once a month to hold on to the new hair.

I was at a hair transplant meeting last week and heard an amazing discussion of cloning that reflects we are closer than I thought to achieving hair cloning. The above link suggests that a drug might regenerate a tooth, certainly on the complexity of a hair follicle. I see a bright future for hair cloning, although getting it through the FDA might take 5+ years once it is achieved. Be patient.