The use of both of these topical medications is effective, as shown here; however, a considerable amount of both of these drugs go systemic. It would be easier to take them orally and then you would know the systemic component of the dosage.

The use of both of these topical medications is effective, as shown here; however, a considerable amount of both of these drugs go systemic. It would be easier to take them orally and then you would know the systemic component of the dosage.
Many men have written to me to ask me if they had Diffuse Unpatterned Alopecia (DUPA), which I defined in the literature with Dr. Bob Bernstein in 1996. This is a “female type of pattern” where the hair in the donor area has significant miniaturized hairs. In men, it is also called Senile Alopecia when appearing in aging men, but here, the hair is uniform in thickness, so miniaturization is not present. The basic premise in hair restoration surgery is that the donor area (a rim of hair about 2 1/2 inches above the ears and around the base of the skull) is privileged hair protected against the genetic of balding. The Norwood Classification shows this area in the Class 7 patterned patient.
The diagnosis is critical because the donor area is no longer protected from the balding process. We don’t believe that DUPA is necessarily inherited, but we don’t know. Sometimes, this donor area miniaturization will respond to finasteride but often does not. If any surgeon dares use this as a source of hair for a hair transplant, the hair transplant will fail, which is a classic malpractice, in my opinion. But for those impacted, controlling their hair loss becomes a real challenge. We have seen the existence of genetic patterned hair loss with DUPA also present, so these men are unfortunately double challenged.
This link shows a classic case of DUPA (https://baldingblog.com/do-i-have-dupa-photo/), so I ask all of my patients to get a hand microscope and cut the hair short in the area, just enough to use the hand microscope and get a good picture as shown in the above post.
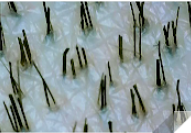
Another man just wrote to me, got a hand microscope, and showed me photos of his donor area. I told him he didn’t have DUPA now, without a doubt. See the photos he sent me below. Very few miniaturized hairs are present, certainly not enough to reach the 20% threshold I use to diagnose DUPA.
I was told that I haven’t lost enough hair to fill in the highlighted areas where I’ve been balding (see outline of my thinning). Do I need to loose more hair to become a better candidate? I consulted two clinics about the number of grafts for my hairline. One said 2000 the other said 2500-2800. Above 2000 seems like too much to me, but I’m not sure. Any feedback is appreciated.
Why undergo a hair transplant if you don’t need it? Hair transplants accelerate balding, especially in younger men. You would likely lose much of the hair presently on your head if there is significant miniaturization present, so maybe a transplant would be switching from what you have to transplanted hair with marginal gain other than the surgeon making money at your expense. There are great medical treatments for your hair if you think you are thinning. Get a doctor that knows how to treat you medically.

I waited for 12 days before washing the recipient area of my transplant. At that time, could I have damaged the grafts?
We wrote an article that discusses what happens day by day after a hair transplant. The grafts are secure in 7-8 days if no crusting is present. If crusting has not come off with good washing, removing the crusts at 12 days with good washing techniques is safe.
I’m 35yrs old living in South East England. Started receding about 10yrs ago and never done anything to prevent it. Only recently started considering a transplant as I’m now starting to be able to afford it.

It will take you at least 6 months to know if it is shock loss, as that is the time it takes to reverse. Now (at 6 weeks) it is too early to tell what will happen. You have every reason to be concerned.


The doctors said this is fine and will grow to look good. Disregarding that its crooked… Does anyone have a similar experience and it turns out more symmetrical later?
It will always be out of balance. What you see is what you get; however, it is not as noticeable when the hair grows in, especially if you style it correctly. If you can’t live with it, this is something I have corrected many times.

I wish I had hair, but I don’t. I am a psychologist and I am trying to understand why being bald impacts my psyche. I spend too much time looking at forums, reading articles and websites to see if I am willing to have a hair transplant, but can’t quite bring myself to do that radical procedure. Lots of horror stories that catch my eye. Your thoughts?
This is a remarkable acceleration of the early effects of topical minoxidil, which shows up in his before picture. Microneedling is most likely responsible for these good early results.


As you can imagine, I’m full bald. I usually shave my head a few times a week and overall I’m not completely unhappy about it. Though, I think it was more curiosity that maybe something amazing could happen and so I’m taking 1mg of fin, and I’ll be using topical minoxidil and I’ve been microneedling for the past month. I’ve also got tretinoin and I’ve been on a serious skin care journey.
I would want to probe your claim of hair loss onset at 12. Showing photos will help. There are hairline changes that occur in some men at 12, but that is not hair loss, but often a maturing hairline. Most men don’t see hair loss until their late teens. This is earmarked by miniaturization in certain impacted hairs, often in the Norwood Classification photos. See an expert to manage the process so that you have a clear idea as to what is happening to you. Do you have a long term plan? Are you considering hair transplants if what you are now doing doesn’t work out?
So I’ve been on finasteride for about 3 years and it’s been great, I also just had a hair transplant about 2 months ago. I started oral minoxidil right after the transplant. On my dad’s side every single man has a full beard, and I personally hate facial hair on me. I like to be well kept and plus I have a nice jawline, I just look better without facial hair. I shave almost twice a day already because of how fast it grows. And oh my lawd, I swear it’s even more thick and grows even more insanely fast ever since I started minoxidil. Actually all my body hair is just growing extremely fast. Will I have to deal with this as long as I’m taking oral minoxidil?
This is the way your body responds to oral minoxidil. It may be the cost you have to pay.
What if I try to enhance the enzyme activity in the scalp with Tretinoin and 1.5mm microneedling. If it still doesn’t respond after combining min tret and microneedling, then maybe I its time to think about oral.
I’m afraid I have to disagree with your logic. If your scalp doesn’t contain Sulfotransferases, then adding Tretinoin may increase some systemic absorption, but 1.5mm microneedling will not make the drug active in the scalp skin. Microneedling may help independently; however, as the liver contains the appropriate enzymes, minoxidil should be effective when taken orally.
I have written extensively on SMP, and it has its limitations: (1) there are significant variables results due to the operator’s skills, (2) variable results due to inks used, (3) fades and changes over time, especially when exposed to sun. SMP works great when used with a hair transplant, as the SMP background impact makes a hair transplant look fuller. I recommend it when my patient has fine hair. I had transplants, for example, and I have fine hair that developed as I got older, so I had SMP done to address this Age Related Thinning problem, see here: https://baldingblog.com/i-just-finished-my-smp-on-my-crown-area-today-see-before-and-after-photos/. Remember, SMP is not hair. The final decision is yours, of course. If you get SMP, ask the person doing it to allow you to meet someone like me who had SMP for 3 or more years. That will tell you if you like what you might be getting.
As only 50% of men have genetic balding, that means that 505 of male models probably are not using any drugs to retain their hair
This is a typical scar healing that I see in many of my patients when I do a strip surgery. These are my pictures (left) 17 days out of surgery (right) 6 months from surgery.

