If you have a tendency to Hypochondriac thinking, then the nocebo effect is clearly something that could impact you. You have to work it out in your own head first, otherwise, sexual side effects will hit you.
Yes, hair loss can come in waves separated by months at times or even years. It can be impacted by your stress and your genetic code
The authors show that the blood flow in the scalp with less hair is less than with more hair. This is because the hair requires a great deal of blood because it has a high metabolic rate. The body pumps blood to the scalp to meet the need to support the high metabolic hair organ system. The reduced blood flow, long held as the cause of hair loss, has never been proven. This is an issue of cause and effect, less hair produces less blood supply not the other way around.
Subcutaneous blood flow in early male pattern baldness
Under an Elsevier user license
open archive
Abstract
The subcutaneous blood flow (SBF) was measured by the 133Xe washout method in the scalp of 14 patients with early male pattern baldness. Control experiments were performed in 14 normal haired men matched for age.
The SBF in the scalp of the normal individuals was about 10 times higher than previously reported SBF values in other anatomical regions. In patients with early male pattern baldness, SBF was 2.6 times lower than the values found in the normal individuals (13.7 ±9.6 vs 35.7 ±10.5 ml/100 g/min?1). This difference was statistically significant (p ? 0.001). A reduced nutritive blood flow to the hair follicles might be a significant event in the pathogenesis of early male pattern baldness.
The answer to this question is possibly, but it needs more investigation. Read this comment published by a notable biologist
No way! Hair is an organ, and therefore transplants from another person will always reject, alive or dead!
Multiple injections into the scalp caused multiple abscesses and hair loss. Make sure you get to see an experienced doctor and not some unskilled doctor who is in the hair filed in it to make a buck! You may pay more heavily than with money for terrible work.

This is an important comment because so many young men want to switch from finasteride to Dutasteride– they feel it is stronger, but this is something I recommend against. Too many young men think that Dutasteride will not give them sexual side effects and they are wrong.
The number of grafts will depend upon (1) the final agreement of where your hairline belongs and what you want (I will assume that the V-shaped hairline is at the lowest point of your mid-line hairline as shown in the photo which should be within 1/2 inch of the highest crease of the furrowed brow), (2) the thickness of your hair (fine, medium or coarse where the finer it is, the more grafts are needed), and (3) the decision to treat the crown with medications rather than a hair transplant reflecting the number range I will give you.
Frontal reconstruction (fine-coarse hair) range would be between 2300-1600 grafts). See this hairline as an example which appears to have more hair loss than you show: https://baldingblog.com/patient-review-from-italian-vacation-photo/
Minoxidil should work on the crown, not sure about the frontal area. Minoxidil will not stop the progression of the frontal balding as finasteride might.

Been to two different consultations now and want to decide between FUT and FUE. Both surgeons I spoke to didnt have a big preference between the two, which I was surprised by. They mentioned that with a skilled surgeon FUT scar shouldn’t be visible, as long as you care for it properly.
The cost difference is significant. For reference I have a really good donor area, NW4. If I have a thin scar in back i really don’t care, as long as it’s not huge.
Second question is that I dont want to take fin. I already have mild ED issues so I don’t want to risk it, neither does my soon to be fiance. Has anyone had success with HT and just minoxidil?
I have written extensively on my website about the differences between FUE and the strip surgery: https://newhair.com/. As the person who pioneered FUE, I am an authority on it. FUE is a great surgery if (1) you have a great surgeon doing it, (2) the surgeon who does it has good judgements on placing the distribution of the FUE excisions so that they are not clumped together and they don’t cause necrosis of the donor area and (3) they know how to handle the grafts to keep them viable for removal and until they are placed back in the head. Add to that, patient selection is critical as people with very fine hair and/or low density often make poor candidates for FUE. I believe that if you are going to develop a very advanced balding pattern, then the strip surgery is better because FUE causes donor site depletion when too many FUE grafts are removed from the donor area as shown here: https://baldingblog.com/collection-victim-photos-internet-harvested-depleted-donor-areas/
I have had 3 strip surgeries and I don’t have a scar that anyone can see. This man had about 4 strip surgeries and a few FUE surgeries and look at his donor area: https://baldingblog.com/norwood-class-7-pattern-patient-received-11000-grafts-plus-smp/. His scars were not very prominent but he had Scalp Micropigmentation just to be sure that nobody would be able to see them as the photos show.
Finasteride will prevent shock loss which is common in young men under 30.
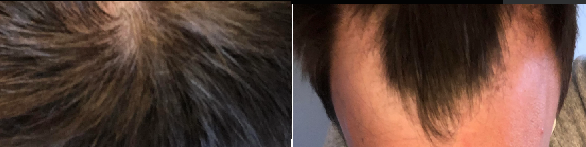
It would be easy to say that the photo on the right had more hair than the photo on the left, but it is all in the lighting as these photos were taken just 20 seconds apart. Too often we want the photos to show us something like more hair, so as you can see here how important consistent lighting and positioning is in photography.

The before picture is below and some benefit can be seen in the upper photo on the left corner of his hairline

I heard that hair loss is dominant trait in males. So if you mother carries the gene you will 100% get it. She is 52 years old and recently started losing alot of hair. Also my grandfather went bald not sure if its because of heart medicine but yeah. Wondering if fpb is the same gene as mpb.
Woman’s hair loss is very different from men’s hair loss. You have a 50/50 chance of inheritance from your mother or dad’s family. Some women get it when they are young especially seen when their mom and sisters got it when they were young. 50% of women get it after menopause when their estrogen levels drop. Estrogen usually protects women from the genes for hair loss and women almost never go bald like some men do.